Download
1 / 28
550 likes | 2.34k Views
Airway Pressure Release Ventilation APRV. By: Jeff Cline, Angie Coon, Randy Hansen November 19, 2012. Scenario.

E N D
Airway Pressure Release VentilationAPRV By: Jeff Cline, Angie Coon, Randy Hansen November 19, 2012
Scenario A new trauma surgeon has arrived at your hospital to direct Surgical Intensive Care. He trained and worked several years at Baltimore Shock Trauma, where they employ Airway Pressure Release Ventilation in many of their patients with ARDS after trauma. He tried to implement APRV on one of his patients and your Respiratory Therapy staff members were not able to assist. He has asked that you develop a protocol for APRV and an educational PowerPoint to inform the staff.
APRV: History and Background • APRV was first described in 1987 by Stock and Downs as a CPAP with an intermittent release phase. 1 • Described as CPAP with intermittent pressure release phase. • Not widely used until it became clinically available in the mid 1990’s • Considered a Rescue Mode of Ventilation in patients with refractory hypoxemia
Other Names for APRV • APRV on Dräger devices • BiLevel on Covidien devices • BiPhasic on CareFusion (formerly Viasys) devices • Bi-Vent on Maquet devices
Advantages/Disadvantages • Advantagesof APRV • Lower Paw for given Vt compared with volume-targeted modes • Lower Ve (less Deadspace Ventilation) • Limited adverse effects on cardio-circulatory function • Decreased sedation use • Near elimination of NMB use (*slide 11) and decrease use of sedation, which translates into decreased length of vent days and ICU length of stay • Disadvantages of APRV • Volume change with alteration in lung compliance and resistance • Process of integrating new technology to staff • Limited access to technology capable of delivering APRV • Limited research and clinical experience
APRV: Who May Qualify/Indications • Patients with a PaO2/FiO2 < 200/300 (ARDS/ALI) and trending downward with increasing oxygen requirements (Refractory Hypoxemia) • Decreasing Lung Compliance with a peak Paw >35cmH2O on conventional ventilatory mode (Plateau Pressure > 30cmH2O) • Patients at Risk for Ventilatory Induced Lung Injury (VILI) • Bilateral diffuse infiltrates on CXR
APRV: Who May Not Qualify/Precautions • Hemodynamic Instability (MAP < 60mmHg)* • Unilateral Lung Disease (i.e. BPF where Independent Lung Ventilation(ILV) may have to be used) • No evidence of Left Atrial Hypertension/CHF (PCWP in ARDS will be < 18mmHg, in CHF > 18mmHg) • Cerebral Edema with Increased Intracranial Pressure • Severe End-Stage COPD
APRV: Goals • Protect the lungs with “Open Lung” concept/strategy • Avoiding VILI due to (I & II : Over distention) • Decreasing Peak Paw • Barotrauma(Alveolar rupture via excessive intrapulmonary pressures) • Volutrauma (Increased epithelial and endothelial permeability via excessive mechanical stretch of the lungs, which may cause pulmonary edema and diffuse alveolar damage) • Atelectrauma (Alveolar damage via repeated opening and closing of the alveoli during the respiratory cycle) • AKA; R.A.C.E. (Repetitive Alveolar Collapse & Expansion) • Shear stress
APRV: Goals (cont) • Protect the lungs with “Open Lung” concept (OLC) • Avoiding VILI due to IV. Biotrauma (RACE May cause systemic inflammation via increasing inflammatory mediators/cytokines, bacterial translocation) • Oxygenate • Recruitment of Alveoli/Preventing Atelectasis/De-recruitment • Increasing FRC and decreasing deadspace ventilation (allowing alveolar units with slow time constants to fill) • Decreasing V/Q shunting and opening Collateral Channels for more homogenous ventilation (via increased meanPaw and spont breathing) • Minimizing oxygen toxicity by raising mean Paw and increasing PaO2/FiO2
APRV: Goals (cont) • Ventilate • Using the patient’s spontaneous efforts to maintain diaphragm strength and mobility through entire respiratory cycle • Relying on the Natural Recoil of the lungs for CO2 elimination(w/out PEEP resisting expiratory flow) with > PEFR’s • Collateral channels of ventilation will be in play (enhanced gas diffusion, requiring 2-3 L’s of Ve < conventional ventilation, suggesting decreased deadspace) • Decrease Work of Breathing (WOB) • Unloading the inspiratory muscles • Improve patient-ventilator synchrony • Reduce the use of Sedation and Paralytics (NMB’s) • Unless NMB’s are used early and limited to 48 hrs on conventional ventilatory mode *(Laurant Papzian, M.D.et al. (2010))
APRV: Goals (cont) • Early weaning off of ventilator • Reducing the risk of Ventilator Associated Pneumonia (VAP)
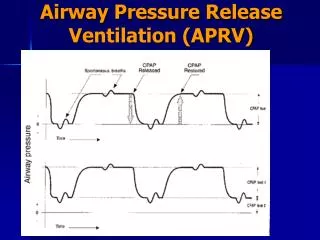
Four Key Settings • P high: The Inflation Pressure • P low: The Deflation Pressure or PEEP • T high: The Inflation Time • T low: The Deflation Time
Initial Settings • P high: Set to plateau pressure of previous conventional ventilation. If new start between 20-30cmH2O pressure. • If extra-thoracic compliance is low, consider target plateau of 30-40cmH2O per physician’s order. • P low: Set to zero. • Allows for peak expiratory phase to remove CO2. • Setting P low above zero may create added resistance with increased turbulent expiratory flow.
Initial Settings • T high: Set between 4-6 secs (rates of 8-12) • For Alveolar Recruitment • T low: Set between 0.2-0.8 secs • Titrate to obtain Peak Expiratory Flow Rate Termination Point at 50-75% of measured Peak Expiratory Flow • Patients with Hx of Obstructive Lung Disease (OLD) should be maintained closer to the 50% Air Trapping • Rise Time, Trigger/Sensitivity, FiO2: • Set per patient comfort, needs and waveform analysis • SpO2 88-92% acceptable • Set all alarms appropriately • Vt’s to be 4-8 ml/kg of IBW
How to Calculate % of Trapped Gas % Trapped Gas = EEF/PEF x 100 ml/sL’s/min 350/1050 x 100 = 33% 38/80 x 100 = 47%
Oxygenation • Increase mean Paw (dependent primarily on P high & T high and may be adjusted simultaneously) • Do not exceed 35cmH2O for P high • Increase P high 2-5cmH2O while assessing patients hemodynamic status • Target up to 30cmH2O • Obtain physician order for P high > 35cmH2O for decreasing trends in overall lung compliance • If oxygenation is poor with a < 50% airtrapping • Decrease T low by increments of 0.05 -0.1 seconds in order to reach target of 75% • If oxygenation is acceptable with a > 75% airtrapping • Increase T low by same increments (0.05-0.1 secs) in order to target 50% trapped gas • Titrate FiO2 to keep SpO2 90-92% (or physician directed)
Ventilation • Assess over-sedation & Spontaneous Frequency • Permit Permissive Hypercapnea with a pH > 7.2 Optimize End-expiratory or Release Lung Volume with… • T low : Increase to allow for more exhaled CO2 time • Stay with the 50-75% air-trapping so oxygenation is not compromised • P high : Increase Vt by increasing by 2-5cmH2O • Target 30cmH2O with Dr’s order for > 35cmH2O • T high : Decreasing will increase your rate of releases/dumps • Do not go < 4 seconds (equivalent to a rate of approximately 12) • Frequency = 60/cycle time (or) 60/(T high + T low) • Patients with high Ve’s may require buffers • Physician may consider bicarb drips or THAM (Tromethamine)
Weaning : “Drop and Stretch” Drop and stretch refers to Dropping the P-High and stretching (increasing) the T-High Weaning of the FIO2 from 100% typically is first though, if pt’s are on higher than normal P-Highs, 35 or > first wean the P-High, then FIO2. As the underlying intrinsic or extrinsic issues start resolving continue to drop FIO2’s then start to drop and stretch. Wean P-Highs slowly to avoid derecruitment, 2-4 every 24hr’s(physician directed). Stretch the T-High .5 to 1 sec when dropping the P-High. Drop and stretch every 12 hours(physician directed). A change to conventional ventilation could be made as P-High are weaned to 16-24, attempting to achieve the same MAP as in APRV
TABLE 4 Example of Airway Pressure Release Ventilation Settings in anUncomplicated Case of Acute Lung Injury43* • Calculated Mean • P High T High P Low T Low Airway Pressure • (cm H2O) (seconds) (cm H2O) (seconds) (cm H2O) • 35 4.0 0 0.8 29.2 • 33 4.5 0 0.8 28.0 • 30 5.0 0 0.8 25.9 • 28 5.5 0 0.8 24.4 • 26 6.0 0 0.8 22.9 • 23 7.0 0 0.8 20.6 • 20 8.0 0 0.8 18.2 • 18 10.0 0 0.8 16.7 • 15 12.0 0 0.8 14.1 • *Following the final settings, the patient was transitioned to CPAP of 12 cm of water pressure. Mean Airway Calculation (P High x T High) + (P Low x T Low) T High + T Low
Extubation • Once P high levels drop to approximately < 16 cmH2O (will vary with institution) and T high is between 12-15 secs (rate about 4-6) and spontaneous respirations account for the majority of the Ve (target 90%) your options are…. • Switch to PSV with ATC (automatic tubing compliance) • Start PEEP at current P high setting and wean to 5-10 prior extubation • May add PS 3-5 cmH2O above PEEP • Continue on APRV with a direct wean • Target P high 8-10 cmH2O with acceptable ABG results • All other evidence based extubation criteria should be used…. • Successful SBT with a RSBI of < 105 for 30-120 minutes with Sedation Holidays • Appropriate LOC/Head lift • Ability to clear secretions/cough • NIF at least -20cmH2O • Ve preferably < 10 l/m • Good clinical judgment !
Concerns About APRV • The very things we are working to avoid by using APRV via the “open lung” strategy, we must also be aware to not create… • Overstretching the lung: Remember that P high is not the only determinant of Vt and that spontaneous breathing causes the pleural pressure to become less positive. Resulting in an increase in the transpulmonary pressure (Alveolar pressure – Pleural pressure) making it easier to take in larger volumes and over-distend the lungs. (Respiratory Care; April, 2007 Vol. 52 No 4) • Atelectrauma: There is concern during the release phase, back to zero, causing derecruitment of lung tissue. Concerned about the “controllability” of this phase. • Lack of Spontaneous Breath: If heavy sedation is needed for comfort, patients will lose the physiologic advantages of APRV; increased venous-return and cardiac output.
Questions? A P R V ?
References Ariel Modrykamien,MD. Robert L. Chatburn, MHHS, RRT-MS. Rendell W. Ashton, MD. Airway pressure release ventilation: An alternative mode of mechanical ventilation in Acute respiratory distress syndrome.(2011). Cleveland Clinic Journal of Medicine, February 2011 vol. 78 2 101-110. Retrieved from; http://www.ccjm.org/content/78/2/101.long Ehab G. Daoud. (2007) Airway Pressure Release Ventilation: Annals of Thoracic Medicine. 2007 Oct-Dec; 2(4): 176-179. Retrieved from; http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2732103/ Laurant Papzian, M.D.et al. (2010) Neuromuscular Blockers in Early Acute Respiratory Distress Syndrome. The New England Journal of Medicine, September 16, 2010 Vol. 363 No.12 P. Milo Frawley, RN, MS, and Nader M. Habashi, MD. (2001). Airway Pressure Release Ventilation: Theory and Practice. AACN Clinical Issues, Volume 12, Number2, pp. 234-246. Retrieved from; http://www.frca.co.uk/documents/HABASHI%20ARTICLE%20APRV.pdf
References • MacIntyre, Neil M.D. (2012). Guidelines for Alternative Modes of Ventilation Used in the Management of Patients with ARDS (September 20, 2012) Retrieved from; www.thoracic.org/clinical/critical-care/salvage-therapies-h1n1/pages/alternative- modes.php • Richey, Scott (2010). APRV Sample Protocol (September 20, 2012). Retrieved from; http://www.aarc.org/resources/adjprot/attc /186/186.pdf • Timothy R Myers RRT-NPS and Neil R MacIntyre MD FAARC. Does Airway Release Ventilation Offer Important New Advantages in Mechanical Ventilator Support? Respiratory Care; April, 2007 Vol. 52 No 4