Download
1 / 105
1.88k likes | 2.91k Views
Wendy Blount, DVM. CPR Update RECOVER. CPR Update. RECOVER. Series of 7 articles in Journal of Veterinary Emergency and Critical Care GOALS evaluate the scientific evidence relevant to small animal CPR compose consensus-based clinical CPR guidelines for dogs and cats. RE assessment

E N D
Wendy Blount, DVM CPR UpdateRECOVER
CPR Update RECOVER • Series of 7 articles in Journal of Veterinary Emergency and Critical Care GOALS • evaluate the scientific evidence relevant to small animal CPR • compose consensus-based clinical CPR guidelines for dogs and cats • REassessment • Campaign • On • VEterinary • Resuscitation.
CPR Update RECOVER – 7 Parts 1 ABOUT “RECOVER” – Materials & Methods 2 Domain 1 - PREPAREDNESS AND PREVENTION Domain 2 - BASIC LIFE SUPPORT (BLS) 3 Domain 3 - ADVANCED LIFE SUPPORT (ALS) 4 5 Domain 4 - MONITORING Domain 5 - POST ARREST CARE 6 CPR GUIDELINES – All 5 domains 7
Wendy Blount, DVM Part 1RECOVER Materials& Methods
Wendy Blount, DVM Domain 1Preparedness and Prevention
Pre-Stocked Arrest Areas Crash Carts • use of both pre-stocked arrest stations and cognitive aids improves compliance with CPR protocols • 80% of GPs and 98% of specialists in VECC & anesthesia have a regularly maintained crash cart • Most problematic are: • missing equipment due to lack of return to the cart • incomplete stocking • Inability to identify or locate needed medications • Failure to have drugs and syringes in a quick, usable form • Deficiencies and defects in resuscitation equipment
Pre-Stocked Arrest Areas Crash Carts • Retrospective study on cardiac arrest in human hospital: • Delay in CPR due to equipment failure 18% of the time • 9% of carts had significant deficiencies • Inaccessible location • Infrequent assessment of cart content • Too much variation in carts when there are more than one • What is the crash cart deficiency rate in vet medicine? • SOLUTIONS: • Checklists and dated log sheet for restocking • Regular re-training of staff • Cognitive Aids improve outcome • flow charts • check lists • Dose charts or calculators
Preparedness Prevention Arrest Etiology & Outcome • anesthesia-related CPAs are associated with increased survival compared to arrests from other causes. • Survival rate of dogs and cats for CPA is between 4 and 9.6% • Survival rate in human hospitals for CPA is 10-20% • Veterinary studies • 36-55% of CPAs occurring under anesthesia survive to discharge • 0-3% of other CPAs survive to discharge • Survive to discharge is much more important than successful CPA resuscitation • Drug reactions resulting in CPA also have a relatively favorable outcome
Preparedness Prevention Arrest Etiology & Outcome • Human studies – operating room CPAs • Death rate 34.9-65.5% for all etiologies of CPA • Death rate 5.5% for anesthesia related CPAs • Human error is noted in 91% of anesthesia related deaths • Post resuscitation debriefing soon after the episode detects and corrects human error.
Preparedness & Prevention CPR Training • CPR skills begin to decay within weeks of training, no matter the learning method used • By 1-2 years after training, skills return to re-training level • Annual CPR training is crucial • Semi-annual CPR training is even better. • American Hospital Association (AHA) • Cognitive performance • completing steps of CPR in an orderly and rapid fashion • Psychomotor skills for BLS • Proper hand position, adequate rate and depth, adequate recoil for chest compressions • Minimizing interruptions • Avoiding excessive ventilation in rate and volume
Preparedness Prevention CPR Team Leadership • Presence of physician at human CPR does not necessarily improve outcome • Some studies show improved outcome, some no difference and a few worse outcome when a doctor is present for CPR • The flaw might be in assuming that physicians are actually more experienced (skilled) than nurses or paramedics at CPR • Survival rates not affected by experience of the first responder • No veterinary studies comparing outcomes of vets vs. techs for CPR • CPR Leadership Training definitely improves outcome of human CPR
Preparedness Prevention CPR Team Leadership • Rapid intervention of the first responder and application of ALS is crucial to improving survival for human CPR • Leadership instruction coordinates the group CPR effort • Technical instruction teaches the mechanics of CPR • CPR Leadership Training improves: • Time to initiate CPR • Percentage of defibrillation within the recommended time window • “hands on time” maximizing CPR time during the emergency • Chest compression rate • Improves cognitive skills • Does not necessarily improve all psychomotor skills
Preparedness Prevention CPR Team Leadership • CPR Leaders are more effective if they do not participate in the resuscitation • CPA simulation is the ideal tool for teaching CPR Leadership • High fidelity manikins with immediate feedback are the best equipment for teaching CPR Leadership skills
Preparedness & Prevention Team Size • Veterinary CPR – Leader (vet or tech) plus three • 1 kennel attendant or tech to ventilate • 1 kennel attendant or tech to do chest compressions • 1 technician to be directed by the leader – intubate, establish IV line, help with cut downs, get supplies and special need items, clean up, etc. • Leader keeps the records and coordinates, doesn’t do anything that takes more than a few seconds • Clear the room of other people, leave the door open, and have others stand by if needed
Preparedness Prevention Standardized Training • Many studies show improved outcome in CPA after standardized training for BLS and/or ALS are implemented • Not widely available in Veterinary Medicine • Case based learning tends to be more effective than text-book training alone • TAMU does provide a first responder paramedical course for veterinary professionals and staff • CPR Guidelines put forth by VECC July 2012
Preparedness & Prevention Debriefing • When high fidelity immediate feedback manikins are not available, post episode debriefing is the next best thing for learning psychomotor skills • Debrief after each real time CPR • Drill, debrief, drill, debrief, drill, debrief • significant improvement in survival in human pediatric patients (33–50%) over time with the use of mock codes and debriefing integrated into a resident teaching program • Patient survival in simulations increased from 0% to 89% during a re-training for ALS certified health care workers, using mock codes and debriefing
Preparedness & Prevention Debriefing • Debriefing is more effective in learning CPR than any other teaching modality used alone • Debriefing can take many forms: • Verbal debriefing • Audio-visual playback and discussion • Review of immediate feedback devices that can record • Computer interactive audio-visual learning modules
Preparedness Prevention Post-Training Assessment • A test at the end of the CPR training session improves learning retention weeks to months later • Reviewing test results can be a learning tool as well.
Preparedness & Prevention Conclusions • In light of the higher survival in dogs and cats following CPA while under anesthesia, consideration should be given to placement of arrest and algorithms in areas where animals are routinely anesthetized • anesthesia induction/prep areas • Surgical suites • Anesthetic recovery areas • At our HQHVSN Clinic, we have 2 surgery tables and one prep table • One table is always open • That table is the arrest station • Crash box is mobile • Emergency drugs are the only drugs not kept in the lock box • Anesthetic arrests most often occur during recovery
CPR Update RECOVER • Key Preparedness and Prevention recommendations for canine and feline CPR • Organized, pre-stocked arrest stations • improve performance • Located where animals are routinely anesthetized • Post-CPR debriefing improves future performance. • Standardized training programs should be developed. • have improved adherence to guidelines in human medicine • are needed in veterinary medicine. • High fidelity manikins are effective in human medicine. • Leadership and team communication training increase • effectiveness.
Wendy Blount, DVM Domain 2BLS – Basic Life Support
Basic Life Support ABC • Establish airway • Ventilation (breathing) • 8-10 breaths per minute if intubated • Up to 20 mm H20 on the manometer • C:V ratio of 30:2 if not intubated (compression:ventilation ratio) • Chest compressions (circulation) • 100 per minute or faster • 1/3 to ½ the width of the chest • Full recoil between compressions (press hard and fast) • Minimize interruptions (no more than 1 every 2 minutes)
Basic Life Support ABC • Numerous studies have shown that the quality of BLS performed is associated with return of spontaneous circulation (ROSC) and survival in arrest victims. • Minimal equipment • Can be started immediately at onset of CPA • Every staff member should be trained in BLS • At least chest compressions and breathing • All may not be able to intubate
Basic Life Support Training • Rapid recognition of CPA • Rapid initiation of CPR • Immediate chest compressions • Begin intubation and ventilation simultaneously
Basic Life Support Training Rapid recognition of CPA • Incidence of CPA during anesthesia • 0.17% in dogs, 0.24% in cats • Patient is unresponsive • Absence of breathing (agonal does not count) • Absence of palpable pulses or auscultable heart sounds • ECG confirms lack of effective circulation If in doubt, do chest compressions • <2% adverse effects when done when not in CPA • Rib fracture, tracheal bleeding, soreness
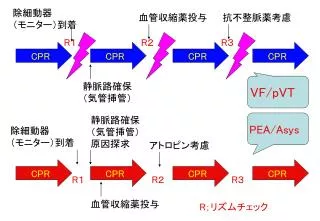
Basic Life Support Training ECG Confirms lack of effective circulation • Asystole • Pulseless ventricular tachycardia • Other pulseless electrical activity • Ventricular fibrillation
Basic Life Support Training Rapid initiation of CPR • One person is the CPR Leader & record keeper • One person does chest compressions unless directed to stop by the Leader • One person establishes the airway and ventilates unless directed to stop by the leader • One person begins ALS, attaches monitors and carries out other tasks as instructed by the CPR Leader
Basic Life Support Training Ventilation • Hypoxia and hypercapnea reduce likelihood or ROSC • Establishing oxygenation may prevent respiratory arrest from progressing to cardiac arrest • When intubation is not available, rescue breathing 30:2 V:C is indicated • Mouth to snout • AmbuBag and snug fitting anesthetic mask • Or anesthetic mask attached to oxygen tank • MAKE SURE VAPORIZER IS OFF • Watch for gastric distension and relieve with manual pressure • Take the manometer to 20 cm H20
Basic Life Support Training Ventilation – Ambu Bags
Basic Life Support Training Ventilation – Ambu Bags
Basic Life Support Training Ventilation – Ambu Bags
Basic Life Support Training Ventilation – Masks
Basic Life Support Training Ventilation – Choosing Reservoir Bag Size (6xTV)
Basic Life Support Training Ventilation – Choosing ET Tube Size (handout)
Basic Life Support Training Ventilation – Tips for endotracheal intubation • Visualize the arytenoid cartilages
Basic Life Support Training Ventilation – Tips for endotracheal intubation • Visualize the arytenoid cartilages • If you didn’t see it go in, assume it’s not in • Use polypropylene catheter stylet for cats (biggest that moves freely in the ET tube – 5Fr, 8Fr, 10Fr) • Use the biggest tube that passes without too much resistance • Fill the cuff, but do not overfill it • Tie the tube in place • Set oxygen flow rate at 1 L/min for circle system (>15 lbs) and 1.5 L/min for non-rebreathing circuits (<15 lbs)
Basic Life Support Training Ventilation – Tips for endotracheal intubation • Trinity Trach Tube Ties – http://trachtubeties.com
Basic Life Support Training Ventilation – Tips for endotracheal intubation • Fiberoptic Laryngoscopes are much superior to bulb laryngoscopes (Miller blades preferred) • Green plastic base on blade, green stripe on handle • Different size attachment than standard laryngoscopes
Basic Life Support Training Chest Compressions • Achieve cardiac output of 25-30% normal • If they generate a pulse, technique is good • circumferential compression vests are not superior to manual compressions at the sternum • Hand placement over the heart for lateral compressions • No evidence that dorsal recumbency is superior to lateral recumbency “Given the lack of high-quality evidence, no evidence based recommendation regarding the best body position for chest compressions in dogs and cats can be made at this time.”
Basic Life Support Training Chest Compressions • Higher compression rates (100-120/min) are associated with better outcome than 60/minute • Do not “lean” on the chest between compressions, to allow full recoil between compressions • Compressions should be fast, as should the release • If you have an extra person, interposed abdominal compressions do improve circulatory resuscitation • Interruptions to check ECG should happen no more often than every 2 minutes
Basic Life Support Training (CPR Flow Sheet Form)
Wendy Blount, DVM Domain 3ALS – AdvancedLife Support
Advanced Life Support • Defibrillation (BLS in CPR for people) • IV fluid therapy to correct metabolic disturbances • Drug therapy, including anesthetic reversal drugs • Open chest CPR • Strong support for epinephrine at 0.01 mg/kg • Strong support for early defibrillation of Vfib or pulseless Vtach • IF BLS and ALS performed promptly, ROSC can be as high as 50%
Advanced Life Support ALS Steps • Apply and respond to Monitors & Vital Signs • HR, RR, temp, ECG, BP, spO2, ETCO2 • IV fluid bolus 10 ml/lb over 10-15 minutes • Contraindicated for congestive heart failure or oliguria/anuria • Reassess and repeat as necessary • Add colloids or hypertonic fluids PRN • Collect blood samples for Quick Assessment Tests • Glucose, BUN, creat, PCV/TS • Run CBC, panel, electrolytes if life can be prolonged • Respond to abnormalities, reassess and respond again
Advanced Life Support Drugs • vasopressors • vagolytics • antiarrhythmics • Glucocorticoids • pH buffers • Reversal agents
Advanced Life Support Drugs Epinephrine – (0.01 mg/kg IV or IT) • Raise blood pressure (pressor) • Improve myocardial perfusion • Increase tissue perfusion • Increase cardiac output (increase SV, increase HR) • This dose is preferred to higher doses
Advanced Life Support Drugs Is Vasopressin preferred to epinephrine? • Dose – 0.8 U/kg IV or IT • Vasopressin causes no additional harm • No studies in dogs and cats to show that vasopressin is better than epinephrine • Vasopressin has an advantage for resuscitation of certain categories of people who suffer CPA • Asystole • Prolonged CPA • Hypovolemia as a cause of CPA
Advanced Life Support Drugs Atropine 1:20 • Dose – 0.4 mg/kg IV or IT • Data using atropine without a pressor are lacking • Reasonable to use when bradycardia or brief asystole occurs due to increased vagal tone • brachycephalics • Ileus, vomiting or other severe GI disease • Respiratory distress • Traumatic intubation • Increased CSF pressure
Advanced Life Support Drugs Atropine 1:20 • Unclear role for prolonged asystole • These need a shock as a last resort • Take care giving atropine when alpha agonists are on board (xylazine, dexdomitor) • Pulmonary hypertension and pulmonary edema • Atropine is not indicated for tachyarrhythmias: • Ventricular fibrillation • Ventricular tachycardia
Advanced Life Support Drugs Antiarrhythmics • Lidocaine** • Procainamide • Amiodarone • Bretylium • Magnesium