Download
1 / 30
340 likes | 594 Views
CPR. What is the correct compression/ventilation ratio for all ages? Is there an exception to this rule?. CPR. 30:2 Yes—15:2 for infants and children with 2 health care providers. CPR. Interruptions to chest compressions should be limited to how long?. CPR.

E N D
CPR • What is the correct compression/ventilation ratio for all ages? • Is there an exception to this rule?
CPR • 30:2 • Yes—15:2 for infants and children with 2 health care providers
CPR Interruptions to chest compressions should be limited to how long?
CPR <10 seconds (unless necessary to intubate or perform another “advanced” skill)
CPR Why is it important to allow for complete chest recoil when performing compressions?
CPR It maximizes venous return of blood to the heart
ACLS List at least 5 signs or symptoms you would associate with “symptomatic” bradycardia.
ACLS • Chest pain • SOB • “Wet” lung sounds (why?) • Cool, clammy skin • Decreased LOC • Hypotension • Weakness or fatigue
ACLS List 5 signs or symptoms you would associate with “symptomatic” tachycardia.
ACLS • Chest pain • SOB • “Wet” lung sounds (why?) • Cool, clammy skin • Decreased LOC • Hypotension • Weakness or fatigue Does this list look familiar?!
ACLS What is the treatment regimen (including doses) for symptomatic bradycardia?
ACLS • ABC’s (don’t forget them!) • O2, IV, monitor • TCP (increase mA until capturing) • Atropine (0.5 mg doses up to 3 mg. max) • Dopamine (2-10 mcg/kg/min) • Epi (2-10 mcg/min)
ACLS List 5 H’s to consider as reversible causes
ACLS • Hypovolemia • Hypoxia • Hypo/hyperkalemia • Hypoglycemia • Hypothermia • Hydrogen ion (acidosis)
ACLS What is the treatment plan (including doses) for narrow complex regular tachycardia with pulses?
ACLS • ABC’s • O2, IV, monitor • Vagal maneuvers • Adenosine (6 mg, followed by 12 mg, and another 12 mg) • Cardioversion if patient is symptomatic
ACLS List 5 T’s to consider as reversible causes
ACLS • Toxins • Tamponade • Tension pneumothorax • Thrombosis (coronary or pulmonary) • Trauma
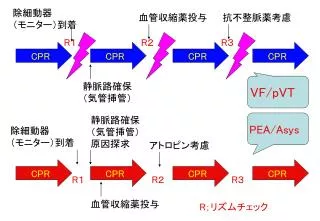
ACLS After determining that a patient is pulseless and not breathing and in VF/VT, list the treatment sequence
ACLS • 1 shock • CPR x2 minutes • Intubation and IV if not already done • Epi 1 mg or Vasopressin 40 U • Re-analyze rhythm and shock PRN • Amio 300 mg or lidocaine 1.5 mg/kg
ACLS After determining that a pulseless, non-breathing patient is in asystole, list the treatment sequence
ACLS • Intubation and IV if not already done • CPR x2 minutes • Epi 1 mg or Vasopressin 40 U • Atropine 1 mg (up to 3 total doses) • Check EKG cables and leads, complex size • Consider termination of efforts
PALS What is the defibrillation dosing sequence for pediatric patients?
PALS 2 joules/kg, followed by 4 joules/kg, followed by 4 joules/kg
PALS What is the “normal” fluid bolus to use for hypotensive infants or children?
PALS 20 cc/kg
PALS What is the formula for determining “normal” BP for children over age 1?
PALS (Age [in years] x 2) + 70
PALS What is the formula for determining uncuffed ETT size in pediatrics? Cuffed tubes?
PALS • (Age [in years] divided by 4) + 4 (uncuffed) • (Age [in years] divided by 4) + 3 (cuffed)