Download
1 / 52
530 likes | 681 Views
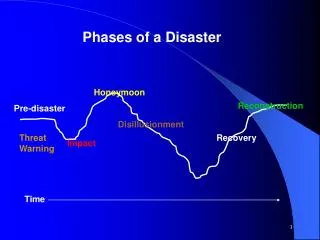
DISASTER DRILLS Help or Hindrance?. Jenny Atas MD FACEP Department of Emergency Medicine Wayne State University March 4 , 2012 Emergencies in Medicine . Effective emergency management takes into account an “all-hazard” approach and includes 4 phases. Mitigation Preparedness Response

E N D
DISASTER DRILLSHelp or Hindrance? Jenny Atas MD FACEP Department of Emergency Medicine Wayne State University March 4 , 2012 Emergencies in Medicine
Effective emergency management takes into account an “all-hazard” approach and includes 4 phases • Mitigation • Preparedness • Response • Recovery
Mitigation According to the Joint Commission on Accreditation of Healthcare Organizations, those activities a hospital undertakes to lessen the impact and severity of a potential emergency.
Preparedness Activities a hospital, healthcare facility or agency undertakes to build capacity and identity resources that may be used if an emergency occurs, such as stockpiles of supplies, personnel, communication tools, etc.
Preparedness Effective emergency management and incident response activities begin with a host of preparedness activities conducted on an ongoing basis, in advance of any potential incident.
Preparedness An integrated combination of assessment, planning, procedures and protocols, training and exercises, personnel qualifications, licensure and certification equipment certification, and evaluation and revision.
Response Involves activation of emergency plans to deal with the actual event .
Recovery Activities designed to help facilities resume normal operations and occurs at the conclusion of the event.
Emergency Management Plans Contingency plans designed to facilitate response and based on a facility’s or agency’s hazard vulnerability analysis (HVA).
Hazard Vulnerability Analysis Purpose: To identify potential emergencies that could affect the need of a facility’s services or affect it’s ability to provide those services.
Elements of a HVA • Define potential risks by developing list of emergencies that may affect a facility’s ability to function including surrounding variables • List of potential internal and external risks (power outages or fires) • Should focus on naturally occurring or manmade disasters, or terrorist or Hazmat incidents
HVA cont. • Assign a probability or likelihood of the event • Rank the severity if the event were to occur • Review the emergency plan to assess how well the facility as well as the community is prepared for a certain type of event • This can be accomplished or rehearsed through various types of drill or exercises
Drills and Exercises • Simulated or based on possible real life scenarios in order to improve response • Based on weakness identified in the HVA
Types of Drills or Exercises • Drill • Tabletop Exercise • Functional Exercise • Full Scale or Field Exercise
Drill A supervised activity with a limited focus to test a component of the emergency management plan, such as an activation notification plan.
Tabletop Exercise • Uses written and verbal scenarios to evaluate the effectiveness of an organization’s emergency management plan • Also focuses on procedures to highlight issues of coordination and assign responsibilities
Functional Exercise • Simulates a disaster in a realistic manner • Utilizes a carefully designed scenario with timed messages between the players and simulators
Full- Scale • Real time • Real equipment • Real responses • Usually involves multiple agencies
Scenario 1Unknown Illness from a Common Source DAY 1 • Flight 3550 with 225 passengers on board lands at your airport • Among the passengers is a group of 100 returning from a 14 day tour of Europe • 75 of the remaining 125 passengers immediately took connecting flights to other states
Scenario 1Unknown Illness from a Common Source DAY 3 • Four (4) members of the tour group began feeling ill and presented to your Emergency Department with high fever, chills, malaise, hypotension and a productive cough. • One (1) patient complains of severe nausea, vomiting, abdominal pain.
Scenario 1Unknown Illness from a Common Source DAYS 4 & 5 • Six (6) more members of the tour group go to area Emergency Departments presenting with similar symptoms as the first group
Scenario 1Unknown Illness from a Common Source DISCUSSION ITEMS • Which agencies exterior to the hospital, if any, should be notified of the current situation, and who is empowered to make that decision? • At what point do you assess that these circumstances may indicate an outbreak? • What resources are available and needed to assist in diagnosing or confirming the diagnosis of an illness? • What are your hospital’s greatest concerns in responding to this type of incident?
Scenario 2Suicide Bomber 7:00 p.m. • Lines at the local Theater Complex have begun filling for the first showing of the evening, and people are beginning to pour into a nearby restaurant adjacent to the theater. As the crowd moves about, a lone man wearing a heavy jacket enters the restaurant. He walks past the hostess and into the center of the dining room where, without hesitating, he detonates a powerful bomb that is hidden beneath his jacket. There is a terrific explosion that demolishes the restaurant. Inside there is momentary silence as debris settles from the collapsed roof. Seconds later a few muffled cries for help can be heard from within.
Scenario 2Suicide Bomber SCENARIO 7:00 p.m. (con’t) • From outside, the front of the building simply disappears behind a brief flash and a hail of smoke and debris. Glass, metal and wood fragments from the restaurant fly through the air injuring scores of people on the sidewalks and along the street in front of the restaurant.
Scenario 2Suicide Bomber SCENARIO 7:01 p.m. • There is pandemonium on the street as the more distant pedestrians instinctively run from the damage. Dozens of people are lying on the street, some injured, some merely stunned. • Moments later, other people run toward the damaged restaurant in an effort to help. Sirens begin to sound in the distance. • The now darkened building and street front is littered with a random mixture of motionless bodies, building materials, human body parts, tables and chairs, and broken glass.
Scenario 2Suicide Bomber SCENARIO 7:05 p.m. to 7:10 p.m. • All hospitals in the area are advised via MedCom radio that a MCI has occurred and asked to activated their external disaster plan. • The hospital receives a call from the first responders on scene, and is informed of the explosion, mass carnage, and that there are approximately 30 Priority-1 victims. • HEICS is initiated. Hospital Command Center is activated. Recall of staff initiated.
Scenario 2Suicide Bomber SCENARIO 7:40 p.m. • Ambulances are arriving at the hospital and the victims are being transported into the ED. 7:45 p.m. • A terrific explosion is felt in the hospital that shakes the walls of the ED. From the main entrance of the hospital there are sounds of panic and screaming. Smoke and dust begin to fill the air. Word comes that a suicide bomber has detonated an I.E.D. in the main visitor reception area and there is massive damage to that area of the hospital and scores of people and staff are injured, many fatally.
Scenario 2Suicide Bomber SCENARIO 7:45 p.m. to 8:15 p.m. • The hospital ED is unable to receive victims and ambulances are diverted to other area hospitals. Police and fire units have secured and stabilized the scene at the hospital and initiated SAR operations. • Available staff begin moving the injured to the ED for triage and treatment. ED staff are quickly overwhelmed and the ED supervisor requests additional personnel. • The ED supervisor advises the I.C. that eight (8) patients need to be transferred to other facilities.
Scenario 2Suicide Bomber DISCUSSION ITEMS • What immediate steps should you take to prepare the Emergency Department Room and staff for this influx of patients? • On a “routine” Saturday night in early summer, what capacity does your ED have to manage a sudden casualty situation of this magnitude? • Given the degree of trauma to these victims, what steps do you need to take at this time of night to ensure that adequate blood supplies are available?
Scenario 2Suicide Bomber DISCUSSION ITEMS • What procedures or protocols exist for handling injured victims who may be suffering from existing medical conditions or diseases such as Hepatitis or HIV/AIDS? • How are large quantities of contaminated tissues, fluids or body parts from mass casualty sites to be handled at your facility?
Scenario 2Suicide Bomber DISCUSSION ITEMS • What special precautions must be taken by EMS and hospital personnel? • What training has your facility’s personnel received in cooperating with and supporting law-enforcement personnel and investigating officers? • What is the immediate responsibility of your ED staff to the arriving victims from the primary terrorist incident, and to those at your own facility?
ARE YOU PREPARED? - - - - - SCENARIO 3 - - - - - • It has been a routine peaceful Sunday in the community and at your hospital. • At 11:00 AM the NWS issues a severe thunderstorm and tornado watch for your area, effective from 2:00 PM until 10:00 PM. • At 4:00 PM the NWS upgrades the severe thunderstorm watch to a warning until 6:00 PM.
ARE YOU PREPARED?------ SCENARIO ------ • At 5:00 PM a severe storm hits your community. • At 5:30 PM the NWS issues a tornado warning for your area. The warning is broadcasted and sirens are activated.
ARE YOU PREPARED?------ SCENARIO ------ • At 5:42 PM a security guard yells, “take cover, a tornado is about to hit the hospital”, and the unthinkable happens… Video Clip Joplin, MO EF-5 Tornado Sunday, May 22, 2011
ARE YOU PREPARED?------ SCENARIO ------ • A minute later here is what’s left of your hospital…
ARE YOU PREPARED?------ SCENARIO ------ • And your community…
ARE YOU PREPARED?------ Initial Response Considerations ------ • Would the HICS be activated at this point? If so, what is the activation process? Which positions would currently be in play? • Would the hospital consider evacuation or SIP at this point? Who would make this decision and based on what critical factors. • What notifications, if any, would you make? • Would you request additional resources at this point? If so, what and from whom?
ARE YOU PREPARED?------ Initial Response Considerations ------ • How will you handle incoming calls from patient family members requesting a situation report? • What other hospital plans, if any, would be activated? • Would your hospital go on diversion? • How will you keep yourselves current regarding the event? • What other actions would you take at this point?
ARE YOU PREPARED?------ SCENARIO UPDATE ------ • The Hospital IC has decided to evacuate the entire hospital as soon as blocked roads are reopened, but for now you are directed to SIP and prepare for evacuation.
ARE YOU PREPARED?------ Response Considerations ------ • What notifications will you make? • Would you call in any additional staff? • What security measures would you take now? • What HICS positions would you consider activating now? • How will you find destinations for your evacuating patients? • How will you coordinate internal patient movement for transportation out of the hospital?
ARE YOU PREPARED?------ Response Considerations ------ • How will you coordinate arriving external transportation to your hospital campus? • How will you track patients as they move throughout your hospital and to the receiving destination? • How will you notify patient family members? Who else needs to be notified? • Will you request any additional resources? From whom? • How will you transfer medical information regarding the patient to the receiving facility?
ARE YOU PREPARED?------ Other Response Considerations ------ • How are you going to handle contaminated patients that self-present to the ED? • How would you surge beyond your internal morgue capacity?
ARE YOU PREPARED?------ Other Response Considerations ------ • How you would get medical supplies and pharmaceuticals if (like Joplin) your internal storage facilities were destroyed? • Do you have plenty of available flashlights and fresh batteries available? (In Joplin the electrical utility went down and the generators were destroyed)
ARE YOU PREPARED?------ Other Response Considerations - Business Continuity ------ • Do you have local access to a disaster field hospital?
August 2, 2011 Medical Response to Joplin Tornado May 22, 2011Immediate Response Considerations • Both incident command centers were destroyed and emergency operations plans (EOP) lost in the debris. Hospitals need deployable incident command centers rather than fixed. • The national exercise occurred just weeks before. The Hospital credits that exercise for the high survival rate and level of preparedness. All presenters talked about the value of exercises and the limited value of written plans. • During your emergency planning process include everyone and do not allow anyone to avoid the planning process, including and especially your medical staff. • Disaster planning and exercises is the key to survival – not the disaster plan.
Special Immediate Concerns Be sure to have a representative in the City/County EOC. Know your local, state, and federal response partners and have an established relationship with them prior to any event. Interoperable communications was an immediate and continuing concern.
Special Immediate Concerns cont’ Hospitals need to consider building bunkers on site to house incident command documents, back up communication resources and emergency supplies; they should be positioned to avoid potential debris fields. The 96 hours of self-sustainability is a myth. The 96-hour cache was consumed in less than 4 hours. Pre-event MOUs and MOAs are good to have in place; however, it may be days before you can communicate with vendors and many may be affected by the event. Your only means of communication for a period of time may be EMS radios. While the hospital is attempting to save lives, EMS crews are engaged in the same battle and may not be available to assist with communications.
Special Immediate Concerns cont’ Is hospital policy written to allow the public to shelter in your facility? Rethink it and plan instead to lock down the facility in the event of a disaster. In an event of this magnitude, the hospital will require armed security. Security forces came in a variety of uniforms, no common identification, and no common radio frequency. Hospitals need the ability to install at least a 6’ steel chain link fence around the perimeter as soon as possible following the initial event.
Lessons Learned Interoperable communication is a must. Hospital and response partners could not communicate effectively. Solar charging stations for cellular phones and radio batteries. Texting/social media worked; all staff should have. Hospital telephone numbers were rolled to PBX system in Springfield, which took 2,500 calls the first day. Long hours w/o relief results in poor decision-making. Manage staff/provide support, including mental health services. Security is critical; you have to protect your resources. Badges will be lost; have wallet identification cards.
Takeaways Know response partners: local, state, federal. Drill with community partners. Have a strong connection with hospital associations. “As leadership goes so goes the staff.” Practice, Practice, Practice. When events occur, EOP documents have very little value. Drill until you fail, then fix it. What you practice is what you do.