Download
1 / 103
1.07k likes | 1.89k Views
Management of the Red Eye. Anthony Cavallerano, OD VA Boston Health Care System New England College of Optometry Boston, Massachusetts Anthony.cavallerano@va.gov. Course Abstract. An overview of anterior segment disorders Review of clinical signs Consideration on differential diagnosis

E N D
Management of the Red Eye Anthony Cavallerano, OD VA Boston Health Care System New England College of Optometry Boston, Massachusetts Anthony.cavallerano@va.gov
Course Abstract • An overview of anterior segment disorders • Review of clinical signs • Consideration on differential diagnosis • Current treatment and management modalities
Red Eye Etiologies • Infection • Inflammation • Irritation • Allergy • Trauma • Chemicals • Tumor • Systemic conditions
Systematic Evaluation of the Red Eye • Orbit • Lids • Lacrimal system • Conjunctiva and sclera • Cornea • Anterior chamber • Iris and pupil • Retina and optic nerve
Red Eye Disorders: Non-Vision Threatening • Blepharitis • Hordeolum • Chalazion • Conjunctivitis • Dry eyes • Corneal abrasions • Subconjunctival hemorrhage
Blepharitis • Colonization of margin with staphylococcus • Classic sign is fibrin collarette • May lead to loss of lashes and margin ulcerations if severe and chronic
Blepharitis • Staph blepharitis may occur with seborrhea. • Often may develop associated problems. • Marginal infiltrates. • Hordeolum. • Chalazion. • Meibomitis. • Marginal infiltrates.
Acute Hordeolum • Acute staph infection of lid • External-glands of Zeiss, moll or lash follicle • Internal- Meibomian • Warm compresses • Systemic antibiotics if preseptal cellulitis develops
Chalazion • Obstruction of Meibomian gland with extrusion of lipid into surrounding tissue • Lipogranulomatous reaction, not infectious • May cause astigmatism secondary to pressure on the cornea
CHALAZION TREATMENT • Most slowly shrink and disappear • Warm compresses • Massage with compression to express contents thru the Meibomian orifice • Oral tetracycline may hasten resolution secondary to its lipid transforming capability • EXCISION usually from conj side
MEIBOMITIS • Meibomian orifice shows erythema and edema with secretions thick and tenacious • Often diffusely inflamed lid margins • Oral teracycline helpful (doxy 100 BID)
STAPH MARGINAL INFILTRATES • Usually non staining discrete limbal infiltrates which are immune mediated and non infectious • Must first rule out infectious keratitis before using steroids • Treat underlying cause ie. blepharitis
Blepharitis treatment • Lid hygiene, as often as possible • Antibiotic ointment to lid margins after cleaning ie. Bacitracin, erythromycin,rarely sulfacetamide • Lubrication often relieves the foreign body sensation which often accompanies the entity
Phlyctenulosis • Round elevated infiltrate which moves centrally from limbus with “leash of vessels” • Sterile type IV hypersensitivity immune rxn , usually to Staph but may be secondary to T.B., or fungal infections
Phlyctenule • Usually resolves spontaneously in 10 –14 days. • Photophobia ,tearing and pain. • Usually leaves pannus and scarring but can rarely perforate. • Topical steroids are used but treating the underling cause is essential.
CONJUNCTIVITIS • Allergic • Viral • Bacterial • Chemical/toxic
Allergic Conjunctivitis • Usually allergy to air born allergen. • Mediated by IgE. • May occur with hay fever, asthma or rhinitis. • Associated with itching, hyperemia, chemosis, watery ,mucoid discharge. • Topical vasoconstrictors and mast cell stabilizers helpful.
VERNAL CONJUNCTIVITIS • Seasonally recurring • History of atopy common • Occurs in children and young adults • Hyperemia and chemosis progress to diffuse papillary hypertrophy on upper tarsus
VERNAL SHIELD ULCER • Localized oval or pentagonal lesion in upper cornea can develop. • Limbal vernal with papilla and Horner-Trantas dots can occur , usually in blacks.
VERNAL CONJUNCTIVITIS • Cold compresses. • Topical vasoconstrictors. • STEROIDS TOPICALLY- usecautiously but often needed since it can be extremely uncomfortable and Va may be decreased. • No steroids in between attacks.
VIRAL CONJUNCTIVITIS • Adenoviral conjunctivitis presents with acute onset of red, watery eyes. • Follicular response worse inferiorly. • Hemorrhagic or pseudomembranous response can occur.
Adenoviral Conjunctivitis • Development of pseudomembranes and symblepharon can occur and delays healing. • Highly contagious and usually lasting 10 days. • Large ,rapidly spreading epidemics.
Adenoviral Keratitis • Represent sterile immunological reactions to viral antigen. Except early • Can produce a severe prolonged subepithelial keratitis which profoundly drops Va
ADENOVIRUS TREATMENT • INFORM patient of 2-4 week course. • May get worse before better. • HIGHLY CONTAGIOUS – precautions. • Tears or topical vasoconstrictors. • Antibiotics if secondarily infected. • Remove pseudomembranes. • Cifovidir? Not FDA approved as of yet. • Topical steroids for SEI’S.
BACTERIAL CONJUNCTIVITIS • HYPERACUTE: Neisseia gonorrhea • Acute catarrhal: s. Pneumonia, Staph, H. . Aegypticus • SUBACUTE: h.Flu • CHRONIC: Staph, Moraxella, pseudomonas,gram negs
Bacterial Conjunctivitis • Mucopurulent discharge. • Broad spectrum antibiotics hasten the resolution. • Must consider gonococcus since it can cause a perforation-hyperacute, needs systemic antibiotics. And has a preauricular node like Adeno.
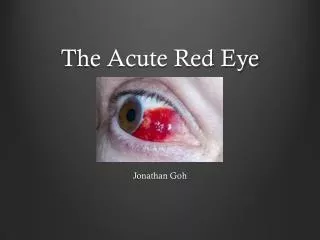
Subconjunctival Hemorrhage • Bright blood red eye. • Normal vision. • No pain. • Usually no obvious cause, often told by others that “eye is red.” • May occur in cases of trauma, or in cases of coughing, vomiting, or straining. • If traumatic must do thorough exam to R/O other pathology.
Subconjunctival Hemorrhage Management • No therapy • Reassurance that the condition is not serious and will resolve in 1-3 weeks • Hematologic coagulation studies are not indicated unless there are associated retinal hemorrhages or many recurrences
Corneal Abrasions • Causes: injury, UV light (welder’s arc), contact lens related, corneal dystrophies, recurrent erosion syndrome, dry eye, corneal anesthesia, infections. • Trauma related abrasions heal very quickly, usually in 24-48 hours. • Recurrent erosions may be sequela of traumatic abrasions.
Corneal Abrasion Therapy • Foster rapid healing • Restore patient comfort • Prevent secondary infections • Topical cycloplegic to relieve pain • Topical antibiotic • +/- Patch, +/- bandage lens
Cornea Abrasion Management • Never patch a contact lens patient due to high risk of infection • Never prescribe topical anesthetics for pain control because of the toxic effects on the corneal epithelium
DRY EYE SYNDROME • Symptoms of tear deficiency include; • FB sensation • Tearing • Ropy mucus • Burning • Scratchiness • ALL WORSE LATER IN THE DAY or in HEAT< WIND OR LOW HUMIDITY
DRY EYE : • Schirmer testing can confirm-5 with,15 without anesthesia in 5 mins. • Rose Bengal staining. • Tear BUT: ,10 secs is definitely abnormal. • Sjogrens syndome is K.Sicca,xerostomia,and arthritis usually in middle aged women. • Tear replacement, plugs, rarely lateral tarsorraphy.
Pinguecula • Benign pathologic change in the bulbar conjunctiva at the palpebral fissure • Associated with sun and wind exposure • Red secondary to increased vascularity of the lesion • Can be intermittently inflamed
Pterygium • Benign change in the bulbar conjunctiva that extends onto the cornea, usually , although not restricted to the medial side of the cornea • Associated with wind and sun exposure • Red secondary to the increased vascularity of the lesion; easily irritated
Pterygium • Wing shaped fold of conj that invades superficial cornea, preceeded by pinguecula. • Increase with proximity to equator. • Elastoid degeneration of collagen with destruction of Bowmans. • Stocker’s line at the head of pterygium.
Pterygium and Pinguecula Treatment • Lubrication - tears • Topical vasoconstrictors • Topical NSAIDs • Topical steroids (not recommended for long term use) • Surgical excision
Surgical Excision : Indications • Encroachment on the visual axis • Induced astigmatism • Chronic irritation • Recurrence rate varies from as high as 50% to as low as 15% • Bare sclera technique without radiation or antifibrotics • Free conjunctival grafts are helpful
Red Eye Disorders: Vision Threatening • Orbital Cellulitis • Scleritis • Uveitis • Trauma • Hyphema • Acute glaucoma • Corneal infections
Preseptal Cellulitis • Inflammation and infection cinfined to periorbital structures anterior to the septum. • In children, underlying sinusitis common eg. H. Flu. • In adults, oftensuperficial skin source is etiology eg. Staph Aureus.
Orbit: Preseptal Cellulitis • Erythema of lids • Edema of lids • Tenderness • Fever • Normal vision • Motility normal • No proptosis
Preseptal Cellulitis Treatment • Systemic antibiotics. • Possible admission for pediatric population with special attention to gram+ coverage and H. Flu. • Adults can be treated with oral antibiotics but watched closely for progression to orbital involvement.
Orbital Cellulitis • Infection extends posterior to the septum • Medical emergency ! • Vision threatening • Life-threatening • Consult with ENT, ophthalmology, infectious disease necessary