Download
1 / 16
180 likes | 709 Views
Case History. Walter Huang, OD Yuanpei University Department of Optometry. Case History. The goal of case history is to obtain an understanding of the patient’s problems and needs

E N D
Case History Walter Huang, OD Yuanpei University Department of Optometry
Case History • The goal of case history is to obtain an understanding of the patient’s problems and needs • It consists of a series of questions to learn about the patient, the purpose for the visit, and the patient’s ocular health history and general health history
Case History • Case history is the most important part of the exam because it guides the exam by helping to narrow down the list of tests that the clinician must do for the remainder of the exam • It offers a good opportunity for the clinician to get to know the patient as a person and build trust with the patient
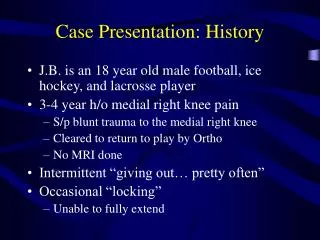
Chief Complaint • The chief complaint is often the first question asked • It is the most important part of the case history because the clinician is trying to determine the purpose for the patient’s visit • It should be an open-ended question • Why did you come in today? • Are you having problems with your eyes?
Chief Complaint • Frequency • How often does this occur? • Constant or intermittent? • Onset • When did the problem begin? • Recent or long-standing? • Location • Where is the problem located? • Right eye, left eye, or both eyes? • Unilateral or alternating?
Chief Complaint • Duration • How long does it last? • Association • What other symptoms do you experience with this problem? • Relief • What seems to make your symptoms go away? • Quality • How would you rate the severity of your symptoms?
Common Eye Problems • Flashes of light • Floaters • Halos around lights • Double vision • Headaches • How often do they occur? • How would you rate their severity? • Eye pain • Redness • Tearing
Visual Demands • Occupation • What kind of work do you do? • Reading • Do you read? • Computer • Do you use the computer? • How many hours per day? • How many days per week?
Visual Demands • Driving • Do you drive? • Do you have problems driving at night? • Hobbies • What are your hobbies? • Sports • What type of sports do you play?
Ocular History • Last eye examination (LEE) • Time • When was your last eye examination? • Location • By whom? • Particular exam findings • What was the outcome of that examination? • Last prescription (LRx)
Ocular History • Glasses • Age • When were your glasses last changed? • Usage • Are they for distance, intermediate, near, or all? • Vision • Describe your vision with your glasses. • Comfort • Describe your comfort with your glasses.
Ocular History • Contact lenses • Average wearing time (AWT) • What is your average wearing time per day? • Wearing time today (WTT) • How long have you worn your lenses today? • Current lens type • What type of lenses do you wear now? • Current lens care regimen • Describe your current lens care regimen, including the solution brand.
Ocular History • Contact lenses • Age • How old are your current lenses? • Usage • Are they for distance? Intermediate? near? or all? • Vision • Describe your vision with your contact lenses. • Comfort • Describe your comfort with your contact lenses.
Ocular History • Ocular diseases • Have you ever been told that you have an eye turn or a lazy eye? • Have you ever been told that you have cataracts (CAT), glaucoma (GLC), or any other eye disease? • Ocular surgeries • Have you ever had any eye surgeries?
Medical History • Last physical examination (LPE) • Time • When was your last physical examination? • Location • By whom? • Particular exam findings • What was the outcome of that examination? • Systemic diseases • Have you ever been told that you have diabetes mellitus (DM), high blood pressure (HTN), thyroid disease, heart disease, or any infectious disease?
Family History Many diseases are highly genetic in nature Specifically ask the patient if any of his family members has diabetes mellitus (DM), high blood pressure (HTN), glaucoma (GLC), strabismus, legal blindness/low vision, or any other disease Record the family member that has each particular disease