Download
1 / 1
10 likes | 167 Views
HPI : 37 year old Male presents via EMS as a ‘Trauma Alert’. He was found face down in his vomit with GCS of 3. Last seen awake and alert 2 hrs ago. EMS reports a strong chemical odor at the scene. Pt was intubated without rapid sequence medications by EMS in the field.

E N D
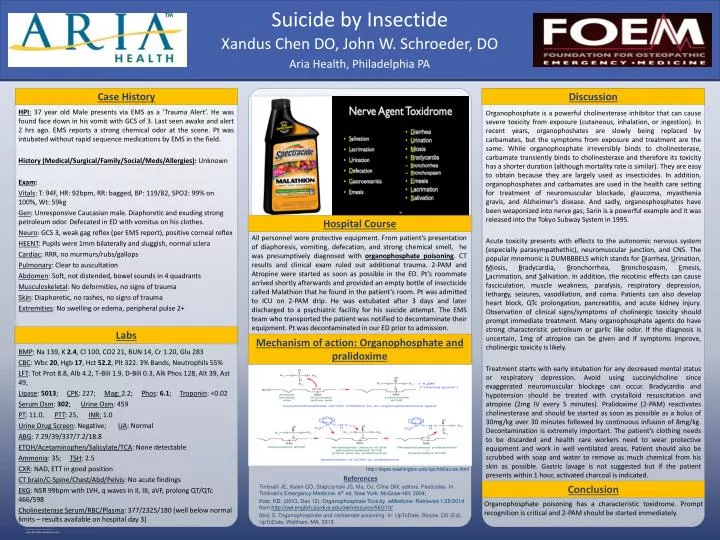
HPI: 37 year old Male presents via EMS as a ‘Trauma Alert’. He was found face down in his vomit with GCS of 3. Last seen awake and alert 2 hrs ago. EMS reports a strong chemical odor at the scene. Pt was intubated without rapid sequence medications by EMS in the field. History (Medical/Surgical/Family/Social/Meds/Allergies): Unknown Exam: Vitals: T: 94F, HR: 92bpm, RR: bagged, BP: 119/82, SPO2: 99% on 100%, Wt: 59kg Gen: Unresponsive Caucasian male. Diaphoretic and exuding strong petroleum odor. Defecated in ED with vomitus on his clothes. Neuro: GCS 3, weak gag reflex (per EMS report), positive corneal reflex HEENT: Pupils were 1mm bilaterally and sluggish, normal sclera Cardiac: RRR, no murmurs/rubs/gallops Pulmonary: Clear to auscultation Abdomen: Soft, not distended, bowel sounds in 4 quadrants Musculoskeletal: No deformities, no signs of trauma Skin: Diaphoretic, no rashes, no signs of trauma Extremities: No swelling or edema, peripheral pulse 2+ Tintinalli JE, Kelen GD, Stapczynski JS, Ma, OJ, Cline DM, editors. Pesticides. In Tintinalli’sEmergency Medicine. 6th ed. New York: McGraw-Hill; 2004; Katz, KD. (2013, Dec 12). Organophosphate Toxicity. eMedicine. Retrieved 1/25/2014 from http://owl.english.purdue.edu/owl/resource/560/10/ Bird, S. Organophosphate and carbamate poisoning. In: UpToDate, Basow, DS (Ed), UpToDate, Waltham, MA, 2013. Case History All personnel wore protective equipment. From patient’s presentation of diaphoresis, vomiting, defecation, and strong chemical smell, he was presumptively diagnosed with organophosphate poisoning. CT results and clinical exam ruled out additional trauma. 2-PAM and Atropine were started as soon as possible in the ED. Pt’s roommate arrived shortly afterwards and provided an empty bottle of insecticide called Malathion that he found in the patient’s room. Pt was admitted to ICU on 2-PAM drip. He was extubated after 3 days and later discharged to a psychiatric facility for his suicide attempt. The EMS team who transported the patient was notified to decontaminate their equipment. Pt was decontaminated in our ED prior to admission. Hospital Course Discussion Organophosphate is a powerful cholinesterase inhibitor that can cause severe toxicity from exposure (cutaneous, inhalation, or ingestion). In recent years, organophoshates are slowly being replaced by carbamates, but the symptoms from exposure and treatment are the same. While organophosphate irreversibly binds to cholinesterase, carbamate transiently binds to cholinesterase and therefore its toxicity has a shorter duration (although mortality rate is similar). They are easy to obtain because they are largely used as insecticides. In addition, organophosphates and carbamates are used in the health care setting for treatment of neuromuscular blockade, glaucoma, myasthenia gravis, and Alzheimer’s disease. And sadly, organosphosphates have been weaponized into nerve gas; Sarin is a powerful example and it was released into the Tokyo Subway System in 1995. Acute toxicity presents with effects to the autonomic nervous system (especially parasympathethic), neuromuscular junction, and CNS. The popular mnemonic is DUMBBBELS which stands for Diarrhea, Urination, Miosis, Bradycardia, Bronchorrhea, Bronchospasm, Emesis, Lacrimation, and Salivation. In addition, the nicotinic effects can cause fasciculation, muscle weakness, paralysis, respiratory depression, lethargy, seizures, vasodilation, and coma. Patients can also develop heart block, QTc prolongation, pancreatitis, and acute kidney injury. Observation of clinical signs/symptoms of cholinergic toxicity should prompt immediate treatment. Many organophosphate agents do have strong characteristic petroleum or garlic like odor. If the diagnosis is uncertain, 1mg of atropine can be given and if symptoms improve, cholinergic toxicity is likely. Treatment starts with early intubation for any decreased mental status or respiratory depression. Avoid using succinylcholine since exaggerated neuromuscular blockage can occur. Bradycardia and hypotension should be treated with crystalloid resuscitation and atropine (2mg IV every 5 minutes). Pralidoxime (2-PAM) reactivates cholinesterase and should be started as soon as possible as a bolus of 30mg/kg over 30 minutes followed by continuous infusion of 8mg/kg. Decontamination is extremely important. The patient’s clothing needs to be discarded and health care workers need to wear protective equipment and work in well ventilated areas. Patient should also be scrubbed with soap and water to remove as much chemical from his skin as possible. Gastric lavage is not suggested but if the patient presents within 1 hour, activated charcoal is indicated. References Xandus Chen DO, John W. Schroeder, DO Suicide by Insectide BMP: Na 139, K 2.4, Cl 100, CO2 21, BUN 14, Cr 1.20, Glu 283 CBC: Wbc20, Hgb17, Hct52.2, Plt 322. 3% Bands, Neutrophils 55% LFT: Tot Prot 8.8, Alb 4.2, T-Bili 1.9, D-Bili 0.3, AlkPhos 128, Alt 39, Ast 49, Lipase: 5013; CPK: 227; Mag: 2.2; Phos: 6.1; Troponin: <0.02 Serum Osm: 302;Urine Osm: 459 PT: 11.0, PTT: 25, INR: 1.0 Urine Drug Screen: Negative; UA: Normal ABG: 7.29/39/337/7.2/18.8 ETOH/Acetaminophen/Salicylate/TCA: None detectable Ammonia: 35; TSH: 2.5 CXR: NAD, ETT in good position CT brain/C-Spine/Chest/Abd/Pelvis: No acute findings EKG: NSR 99bpm with LVH, q waves in II, III, aVF, prolong QT/QTc 466/598 Cholinesterase Serum/RBC/Plasma: 377/2325/180 (well below normal limits – results available on hospital day 3) Labs Mechanism of action: Organophosphate and pralidoxime Conclusion Aria Health, Philadelphia PA http://depts.washington.edu/opchild/acute.html Organophosphate poisoning has a characteristic toxidrome. Prompt recognition is critical and 2-PAM should be started immediately.