Download
1 / 1
10 likes | 166 Views
CAN ILIOPSOAS MUSCLE CONTRIBUTE STIFF KNEE GAIT PATTERN? A PRELIMINARY STUDY. Ekin N. Akalan 1,4, Shavkat N. Kuchimov 2, Adnan Apti 3 and Yener Temelli 4 . 1.Istanbul University, Faculty of Health Science, Physiotherapy and Rehabilitation Division and

E N D
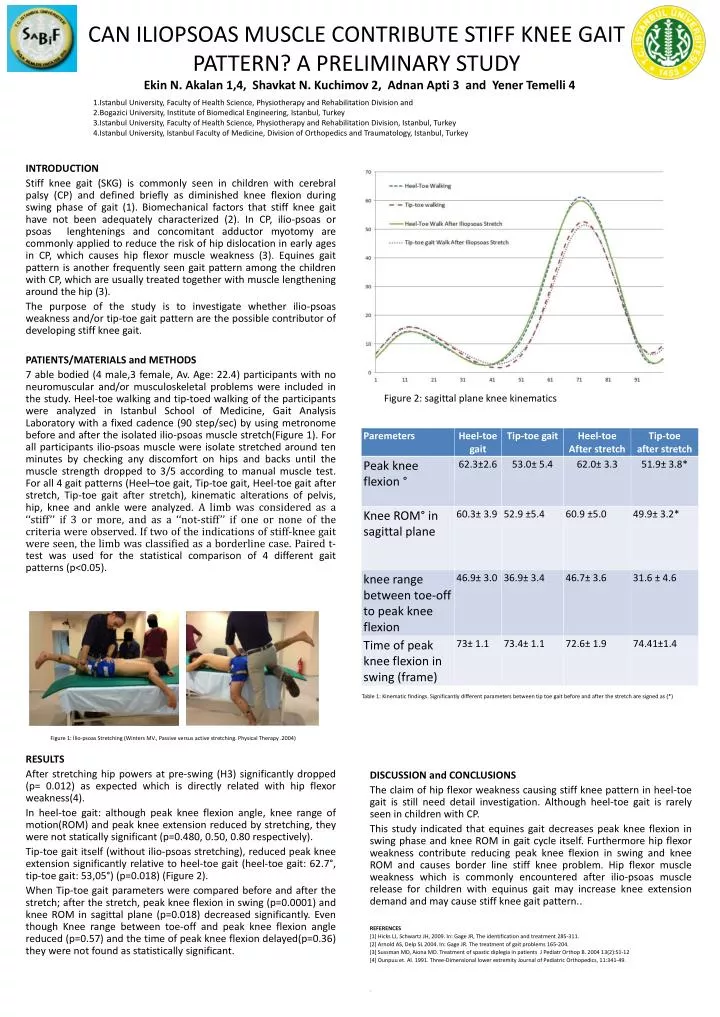
CAN ILIOPSOAS MUSCLE CONTRIBUTE STIFF KNEE GAIT PATTERN? A PRELIMINARY STUDY Ekin N. Akalan 1,4, Shavkat N. Kuchimov 2, Adnan Apti 3 and Yener Temelli 4 1.Istanbul University, Faculty of Health Science, Physiotherapy and Rehabilitation Division and 2.Bogazici University, Institute of Biomedical Engineering, Istanbul, Turkey 3.Istanbul University, Faculty of Health Science, Physiotherapy and Rehabilitation Division, Istanbul, Turkey4.Istanbul University, Istanbul Faculty of Medicine, Division of Orthopedics and Traumatology, Istanbul, Turkey INTRODUCTION Stiff knee gait (SKG) is commonly seen in children with cerebral palsy (CP) and defined briefly as diminished knee flexion during swing phase of gait (1). Biomechanical factors that stiff knee gait have not been adequately characterized (2). In CP, ilio-psoas or psoas lenghtenings and concomitant adductor myotomy are commonly applied to reduce the risk of hip dislocation in early ages in CP, which causes hip flexor muscle weakness (3). Equines gait pattern is another frequently seen gait pattern among the children with CP, which are usually treated together with muscle lengthening around the hip (3). The purpose of the study is to investigate whether ilio-psoas weakness and/or tip-toe gait pattern are the possible contributor of developing stiff knee gait. PATIENTS/MATERIALS and METHODS 7 able bodied (4 male,3 female, Av. Age: 22.4) participants with no neuromuscular and/or musculoskeletal problems were included in the study. Heel-toe walking and tip-toed walking of the participants were analyzed in Istanbul School of Medicine, Gait Analysis Laboratory with a fixed cadence (90 step/sec) by using metronome before and after the isolated ilio-psoas muscle stretch(Figure 1). For all participants ilio-psoas muscle were isolate stretched around ten minutes by checking any discomfort on hips and backs until the muscle strength dropped to 3/5 according to manual muscle test. For all 4 gait patterns (Heel–toe gait, Tip-toe gait, Heel-toe gait after stretch, Tip-toe gait after stretch), kinematicalterations of pelvis, hip, knee and ankle were analyzed. A limb was considered as a ‘‘stiff’’ if 3 or more, and as a ‘‘not-stiff’’ if one or none of the criteria were observed. If two of the indicationsof stiff-knee gait were seen, the limb was classified as a borderline case. Paired t-test was used for the statistical comparison of 4 different gait patterns (p<0.05). RESULTS After stretching hip powers at pre-swing (H3) significantly dropped (p= 0.012) as expected which is directly related with hip flexor weakness(4). In heel-toe gait: although peak knee flexion angle, knee range of motion(ROM) and peak knee extension reduced by stretching, they were not statically significant (p=0.480, 0.50, 0.80 respectively). Tip-toe gait itself (without ilio-psoas stretching), reduced peak knee extension significantly relative to heel-toe gait (heel-toe gait: 62.7°, tip-toe gait: 53,05°) (p=0.018) (Figure 2). When Tip-toe gait parameters were compared before and after the stretch; after the stretch, peak knee flexion in swing (p=0.0001) and knee ROM in sagittal plane (p=0.018) decreased significantly. Even though Knee range between toe-off and peak knee flexion angle reduced (p=0.57) and the time of peak knee flexion delayed(p=0.36) they were not found as statistically significant. DISCUSSION and CONCLUSIONS The claim of hip flexor weakness causing stiff knee pattern in heel-toe gait is still need detail investigation. Although heel-toe gait is rarely seen in children with CP. This study indicated that equines gait decreases peak knee flexion in swing phase and knee ROM in gait cycle itself. Furthermore hip flexor weakness contribute reducing peak knee flexion in swing and knee ROM and causes border line stiff knee problem. Hip flexor muscle weakness which is commonly encountered after ilio-psoas muscle release for children with equinus gait may increase knee extension demand and may cause stiff knee gait pattern.. REFERENCES [1] Hicks LJ, Schwartz JH, 2009. In: Gage JR, The identification and treatment 285-311. [2] Arnold AS, Delp SL 2004. In: Gage JR. The treatment of gait problems 165-204. [3] Sussman MD, Aiona MD. Treatment of spastic diplegia in patients J PediatrOrthop B. 2004 13(2):S1-12 [4] Ounpuu et. Al. 1991. Three-Dimensional lower extremity Journal of Pediatric Orthopedics, 11:341-49. : Figure 2: sagittal plane knee kinematics Table1: Kinematicfindings. Significantlydifferentparametersbetween tip toegaitbeforeandafterthestretcharesigned as (*) Figure 1: İlio-psoasStretching (Winters MV., Passiveversusactivestretching. PhysicalTherapy .2004)