Download
1 / 16
200 likes | 683 Views
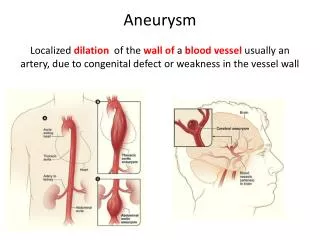
Angina pharmacology. Summary. Drugs Stable angina management: reduce heart O 2 demand Nitrates (reduce venous return) Beta blockers (reduce sympathetic drive) Calcium channel blockers (reduce inotropic state) Refractory stable angina options Perhexiline , Ivabradine

E N D
Summary • Drugs • Stable angina management: reduce heart O2 demand • Nitrates (reduce venous return) • Beta blockers (reduce sympathetic drive) • Calcium channel blockers (reduce inotropic state) • Refractory stable angina options • Perhexiline, Ivabradine • Preventative agents • Thrombosis prophylaxis(Aspirin, clopidigrel, dipyrimadole, heparins) • Statins • ACE inhibitors • Diuretics
Triple Whammy ACE Inhibitor, diuretic, and NSAID: a dangerous combination (TGA.gov.au, Australian Adverse Drug Reactions Bulletin 2003) • NSAID + Diuretic + ACE inhibitor • Correlation with Renal failure • ADRAC wishes to remind prescribers that the combination of ACE inhibitors (or angiotensin receptor antagonists), diuretics and NSAIDs (including COX-2 inhibitors) should be avoided if possible, and great care should be taken with ACE inhibitors and NSAIDs in patients with renal impairment.
Nitrates • Mechanism • Release nitric oxide (NO) • NO dilates venules and coronary arteries • Increases venous capacitance • Decreases preload • Decreases contractility (Frank-Starling mechanism)
Nitrates • Adverse effects • Headaches, hypotension, flushing, palpitations, orthostatic hypotension, fainting, peripheral oedema, contact dermatitis • Contraindications • Hypovolemiaor hypotension • Raised intracranial pressure • Significant anemia • G6PD deficiency (risk of hemolyticanemia) • Recent (1-5 days) use of PDE5 inhibitors (excacerbates hypotension) • hypertrophic obstructive cardiomyopathy • cardiac tamponade • Aortic stenosis, mitral stenosis, corpulmonale. • Precautions • Tolerance. 10-12 hour nitrate free interval recommended each day. • Withdrawal. Reduce dose gradually.
Nitrates Nicorandil Also opens KATP channels in smooth muscle, dilating arterial as well as venous vessels. Can cause ulcers, often in the mouth.
Nitrates Australian Medicines Handbook
β-blockers • Competitively antagonise beta adrenergic receptors • Blunt sympathetic stimulation • Reduce contractility and rate • No reflex rise in peripheral resistance
β-blockers • Contraindications • Reversible airway disease • Cardiogenic and hypovolemic shock • Prinzmetal (vasospasm) angina • Bradycardia, 2nd and 3rd degree Heart block, Sick sinus • Adverse effects • nausea, diarrhoea, bronchospasm, dyspnoea, cold extremities, exacerbation of Raynaud's syndrome, bradycardia, hypotension, orthostatic hypotension (carvedilol, labetalol), heart failure, heart block, fatigue, dizziness, abnormal vision, decreased concentration, hallucinations, insomnia, nightmares, depression, alteration of glucose and lipid metabolism, oedema (carvedilol) • Precautions • Diabetes: hypoglycemia sign can be masked • Hyperthyroidism: signs masked • Anaphylaxis risk: Reduces epipen effect • Phaeochromocytoma: aggravates hypertension • Myasthenic symptoms: aggravated • Peripheral vascular disease or Raynaud’s phenomenon: aggravated • Renal or hepatic impairment: Choose drug with appropriate elimination route
β-blockers for angina Australian Medicines Handbook
L-type Calcium channel blockers • Dihydropyridines • Strong vasodilation (arterial) • Decreases afterload • Phenylalkylamine • Verapamil • (less) Vasodilationand (more) cardiac depression • Decreases afterload, heart rate, and contractility • Benzothiazepine • Diltiazem • (more) Vasodilationand (less) cardiac depression • Decreases afterload, heart rate, and contractility
L-type Calcium channel blockers • Contraindications • Cardiogenic shock, Heart failure, Aortic stenosis • Adverse effects • Transient worsening of angina symptoms • Reflex tachycardia (short acting dihydropyridines) • Bradycardia(Diltiazem, Verapamil) • Headache, flushing, peripheral oedema (especially dihydropyridines) • Gingival hyperplasia • Constipation (Verapamil) • Rash, fatigue, dizziness, nausea, abdominal pain • Precautions • Myasthenia-like disease – exacerbated symptoms • Avoidβ blockers with Verapamil • Useβ blocker with dihydropyridines? (Murtagh) • CCB related oedema may not respond to diuretics
L-type Calcium channel blockers Australian Medicines Handbook Nimodipineis a CCB indicated for subarachnoid hemorrhage management
Refractory stable angina options PerhexilineAustralian Medicines Handbook
Saturable hepatic metabolism • Australian Medicines Handbook – Drugs and CYP enzymes • Cytochrome P450 enzyme family • CYP1A2 • CYP2B6 • CYP2C8 • CYP2C9 • CYP2C19 • CYP2D6 • CYP3A4/5 • Interactions • Grapefruit, Starfruit , St John’s Wort, Nicotine, Watercress • Pharmaceuticals
Refractory stable angina options IvabradineAustralian Public Assessment Report for IvabradineAustralian Medicines Handbook