Download
1 / 37
400 likes | 415 Views
Dr. Mohammed Kalimi. Thyroid Physiology. Iodide Turnover. Input = Output 500 μ g Iodide = Renal excretion =480 μ gI - (Daily dietary) Stool excretion= 20 μ g I -. Biosynthesis of TH. 1. Iodide pump or trap:

E N D
Dr. Mohammed Kalimi Thyroid Physiology
Iodide Turnover • Input = Output • 500 μg Iodide = Renal excretion =480 μgI- (Daily dietary) Stool excretion= 20 μg I -
Biosynthesis of TH • 1. Iodide pump or trap: • Transport of iodide into the gland against electro chemical gradients by Na+ -I- cotransport (symport) • ↑ Na-K ATPase and TSH • Inhibition by Sodium thiocyanate and Perchlorate
T/S Ratio • Normal T/S 20:1 • TSH stimulation 100:1 • Hypophysectomized (no TSH) 1:1
Biosynthesis of TH • 2. Conversion of Iodide to Iodine 2I - I2 • H2O2 sustrate and thyroid peroxidase enzyme • ↑ TSH and inhibited by PTU and methimazole
Biosynthesis of TH • 3. Organification: Formation of MIT and DIT by iodination of tyrosyl residue of TG • 4. Coupling: MIT + DIT = T3 DIT + DIT = T4 Organification and coupling are caralyzed by thyroid peroxidase and require hydrogen peroxide and TSH
Administration of large quantities of Iodide (2 mg or more) • TH synthesis due to • expression of Na-I symporter • enzyme peroxidase genes
T3 and T4 Plasma bound T4 = 99.97% Plasma free T4 = 0.03% Plasma bound T3 = 99.7% Plasma free T3 = 0.3%
T3 and T4 • Ten times (of the total) T3 in the blood is free Compared to T4 • Plasma half life of T3 = 1 day • Plasma half life of T4 = 7 days • T3 is two to three times more biologically potent than T4
TH blood binding proteins • Thyroxine binding globulins (TBG): binds to about 70% total T4 and 50% total T3 • Thyroxine binding prealbumin (TBPA): binds 20% of total T4 ( no binding to T3) • Albumin : binds 10% of total T4 and 50% of total T3
Degradation of T4 • 1. Conversion of T4 to T3 (T4 5’ Deiodinase T3) about 35% • 2. Conversion of T4 to rT3 (T4 5 Deiodinase rT3) about 45% • 3. T4 metabolised by cojugation or oxidative deamination : about 20%
Reverse T3 • Physiological role unknown • Levels ↑ with chronic illness, calorie deprivation, β blockers and corticosteroids
Thyroid Physiology • Acts on most tissues • Action –slow in onset and long in duration • TH is not necessary for life, improves quality of life
TH Actions • 1. Growth and Development • 2. Metabolic • 3. Neural • 4. Cardiovascular
TH Actions • Normal growth (↑GH)and development (bone, skeletal and brain) • Congenital deficiency ; cretinism • Dwarf stature (bone remains infantile ), mental retardation
TH Actions • Metabolic: ↑ BMR, ↑ O2 consumption, ↑ heat production, ↑ mitochondrial ATP synthesis. • Acute response to cold by ↑ BMR, ↑ heat production, ↑ catecholamines, ↑ lipolysis, ↑ cardiac adjustments, ↑ muscular activity • Chronic cold: ↑ conversion of T4 to T3
TH Actions • ↑ Carbohydrate, protein and lipid metabolism • ↑ Gluconeogenesis, ↑ Glycolysis, ↑ absorption of carbohydrates from the GI tract • Negative nitrogen balance (↑ protein turnover) • ↑ Lipolysis, FFA synthesis and oxidation • Total cholesterol and LDL
TH Actions • Neural: Promotes normal neuronal development • Cardiovascular effects: ↑ heart rate and strength of the heart beat, ↑ ventilation and cardiac output • ↑ Cardiac β receptors
TRH • Tripeptide • Synthesized and released from hypothalamus • ↑ T3,T4, anterior pitutary TRH receptors, TSH
TSH • α subunit identical with LH, FSH, hCG • β subunit is specific to TSH • Plasma T1/2= 1 hour • Plasma TSH levels = 0.5-5.0 μU/ml • ↑ TSH, ↑ cold, ↑ TRH, ↑ leptin • TSH, sleep, fasting and ↑ somatostatin
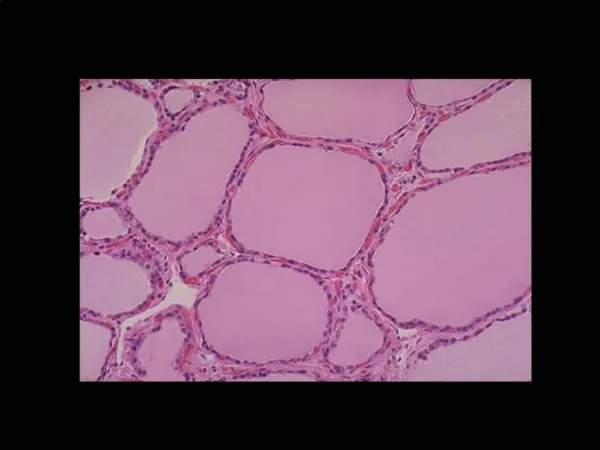
Goiter ( enlargement of TH gland) • Prolonged and excessive TSH stimulation of TH gland • Euthyroid Goiter: Iodide deficiency, ↑ TSH to compensate TH • Hyperthyroid Goiter: over secretion of TSI (thyroid stimulating immunoglobulin) which mimics TSH, ↑ TSI, ↑TH • Hypothyroid Goiter: Administration of drugs such as PTU, perchlorate, thiocyanate, TH,↑ TSH
TH : Clinical tests • Measurement of plasma total T3 and Total T4 • Measurement of TSH • Normal values= 0.5-5.0 micro units/ mL of blood • Elevation in serum TSH is the most sensitive measure for primary hypothyroidism
TH: Clinical tests • TSH above 5.0 (hypothyroidism) treatment with thyroxine • TSH below 0.5 (hyperthyroidism), radiation treatment plus thyroxine (T4)
TH Clinical • In deficiency state: Hypothyroidism • Overactivity: Hyperthyroidism
Hypothyroidism • Primary disease: Thyroid failure (surgical, immune or iodide destruction of thyroid gland) • Secondary disease: Pituitary (TSH deficiency) or hypothalamus (TRH deficiency)failure • Defective TH receptors • Myxedema • Cretinism
Symptoms of hypothyroidism • Decreased BMR , decreased pulse rate and vitality • Increased plasma cholesterol and LDL • Growth failure, weight gain, constipation • Dry scaly thickened skin, cold intolerance • Sluggishness, hoarse voice, lethargic, puffy eyelids, enlragement of tongue • Depression and insomnia
Hyperthyroidism • Graves’ disease (Thyrotoxicosis) • ↑ TSI, ↑ T3,T4, TSH
Symptoms of hyperthyroidism • ↑ BMR • Plasma Cholesterol and LDL • ↑ Cardiac output, ↑ heart rate and ↑cardiac beta receptors, congestive heart failure • ↑ Body heat, sweating and vasodialation • Osteoporosis (negative calcium balance) • Hyperkinetic and psychotic behavior • ↑ GI malfunctions and weight loss • Neuro muscular-fatigue,hyperactive reflexes • Eye discomfort, marked protrusion of eyes (exophthalamos)
Pregnancy and TH • Pregnancy, ↑ Estrogen, ↑TBG, ↑Total plasma T3 and T4