Download
1 / 67
720 likes | 880 Views
Status Epilepticus. Zohair A. Al Aseri MD, FRCPC EM & CCM Associate Professor , DEM and CCD College of Medicine King Saud University Consultant Emergency Medicine and Intensivist King Saud University Medical City. References. Status Epilepticus.

E N D
Status Epilepticus Zohair A. Al Aseri MD, FRCPC EM & CCM Associate Professor , DEM and CCD College of Medicine King Saud University Consultant Emergency Medicine and Intensivist King Saud University Medical City Zohair Al Aseri MD,FRCPC EM & CCM
References Status Epilepticus • Evidence-Based Guideline: Treatment of Convulsive Status Epilepticus in Children and Adults: Report of the Guideline Committee of the American Epilepsy Society. Tracy Glauser et al. / Epilepsy Current. • Challenges in the treatment of convulsive status epilepticus. G. Zaccara et al. / Seizure 47 (2017) 17–24 • 25 years of advances in the definition, classification and treatment of status epilepticus. E. Trinka, R. Kälviäinen / Seizure 44 (2017) 65–73 • Billington, M.; Kandalaft, O.R.; Aisiku, I.P. Adult Status Epilepticus: A Review of the Prehospital and Emergency Department Management. J. Clin. Med. 2016, 5, 74. • https://emcrit.org/pulmcrit/rapid-sequence-termination-rst-of-status-epilepticus/ Zohair Al Aseri MD,FRCPC EM & CCM
Status Epilepticus Objectives • Introduction & Definitions • Causes • Investigation • Evidence-Based treatment options • Algorithm • Conclusion Zohair Al Aseri MD,FRCPC EM & CCM
Introduction • High morbidity and mortality. • SE is a manifestation of a disease. It is mandatory to look for an underlying cause Higher rate of complications including permanent neuronal damage Prolonged Seizure DeLorenzo R.J., Hauser W.A., Towne A.R., et al: A prospective, population-based epidemiologic study of status epilepticus in Richmond, Virginia. Neurology 46. (4): 1029-1035.1996; Zohair Al Aseri MD,FRCPC EM & CCM
Status Epilepticus New Definitions SE: Refractory SE RSE: (ILAE Task force), 2015 Seizure that is prolonged after initiation of mechanisms to terminate the seizure within 5 minutes SE that persists despite adequate administration of benzo. and at least one antiepileptic drug Holtkamp M: Treatment strategies for refractory status epilepticus. Curr Opin Crit Care 17. 94-100.2011 Novy J, Logroscino G, Rossetti AO: Refractory status epilepticus: a prospective observational study. Epilepsia 51. 251-256.2010 Trinka E., Cock H., Hesdorffer D. A definition and classification of status epilepticus—Report of the ILAE Task Force on Classification of Status Epilepticus. Epilepsia. 2015;56:1515–1523. doi: 10.1111/epi.13121 Zohair Al Aseri MD,FRCPC EM & CCM
Why there is no mentioning about seizure termination with benzo in the 1st 5 minutes of SE management???? Wahts wrong with this algorithm What about the definition Zohair Al Aseri MD,FRCPC EM & CCM
Billington, M.; Kandalaft, O.R.; Aisiku, I.P. Adult Status Epilepticus: A Review of the Prehospital and Emergency Department Management. J. Clin. Med. 2016, 5, 74. Zohair Al Aseri MD,FRCPC EM & CCM
Status epilepticus presents in several forms: focal motor signs, focal sensory symptoms, or focal impairment of function (e.g aphasia) not associated with altered awareness (epilepsiapartialis continua). repeated generalized tonicclonic seizures with persistent postictal depression of neurologic function between seizures Convulsive status epilepticus Nonconvulsive status epilepticus seizures produce a continuous or fluctuating “epileptic twilight” state Repeated partial seizures Zohair Al Aseri MD,FRCPC EM & CCM
Vascular StrokeSAHSub or Epidural HematomaVasculitis Infectious MeningitisEncephalitisBrain abscess Metabolic HyponatremiaHypoglycemiaHypocalcemiaHypo Mg Toxic CocaineTricyclicsAnticholinerg. IsoniazidWithdrawal TumorsEclampsia Zohair Al Aseri MD,FRCPC EM & CCM
Status Epilepticus Initial stabilization Simultaneously: • Oxygenation and ventilation • IV access • Antiepileptic • Glucocheck • Diagnostic studies • Thiamine, 100 mg for alcohol abuse pt. • Empiric AB, ceftriaxone, 1 to 2 g IV and vancomycin, 1 g IV if you suspect CNS infection. Zohair Al Aseri MD,FRCPC EM & CCM
Status Epilepticus if intubation needed: Initial stabilization • RSI • Paralytic agents will stop the motor activity but not the abnormal neuronal firing SE. • Use ketamine and propofol Zohair Al Aseri MD,FRCPC EM & CCM
Ketamine for the treatment of refractory status epilepticus. Y. Fang, X. Wang / Seizure 30 (2015) 14–20 Zohair Al Aseri MD,FRCPC EM & CCM
https://emcrit.org/pulmcrit/rapid-sequence-termination-rst-of-status-epilepticus/https://emcrit.org/pulmcrit/rapid-sequence-termination-rst-of-status-epilepticus/ Zohair Al Aseri MD,FRCPC EM & CCM
Status Epilepticus Diagnostic testing Laboratory Studies • Serum electrolytes • Ca, Mg • Glucose • Renal and Liver function testing • Antiepileptic drug levels • Toxicology screen Zohair Al Aseri MD,FRCPC EM & CCM
Diagnostic testing Status Epilepticus Neuroimaging • A noncontrast Brain CT should be considered for all SE patients once they have been stabilized. Lumbar Puncture if you suspect CNS infection • Empiric antibiotic or antiviral therapy • Obtain CT Zohair Al Aseri MD,FRCPC EM & CCM
Status Epilepticus Diagnostic testing EEG Monitoring • Nonconvulsive SE. • Comatose after generalized seizure • Paralytics where neuro examination is impossible Zohair Al Aseri MD,FRCPC EM & CCM
Treatment Anticonvulsant selection depends on “efficacy” Ability to stop convulsive SE. “tolerability” “incidence, severity and impact” of adverse effects. “effectiveness” Bothefficacy and tolerability. “safety” life-threatening adverse events. Few RCT that demonstrate superiority of one agent over another. Zohair Al Aseri MD,FRCPC EM & CCM
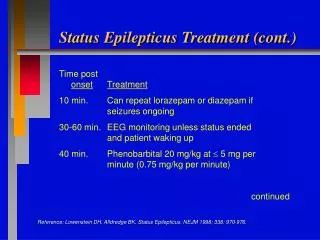
Status Epilepticus Treatment Benzodiazepines The first drugs of choice for SE. • Diazepam (0.2 mg/kg given at 5 mg/min) • Lorazepam (0.1 mg/kg given at 2-4 mg/min) Zohair Al Aseri MD,FRCPC EM & CCM
Basic principles of SE treatment • Benzodiazepines are the only evidence-based treatment, as shown in three trials and a Cochrane review. • Treiman DM, Meyers PD, Walton NY, et al: A comparison of four treatments for generalized convulsive status epilepticus. Veterans Affairs Status Epilepticus Cooperative Study Group. N Engl J Med 339. 792-798.1998; • Alldredge BK, Gelb AM, Isaacs SM, et al: A comparison of lorazepam, diazepam, and placebo for the treatment of out-of-hospital status epilepticus. N Engl J Med 345. 631-637.2001; • Leppik IE, Derivan AT, Homan RW, Walker J, Ramsay RE, Patrick B: Double-blind study of lorazepam and diazepam in status epilepticus. JAMA 249. 1452-1454.1983; • Prasad K, Al-Roomi K, Krishnan PR, Sequeira R: Anticonvulsant therapy for status epilepticus. Cochrane Database Syst Rev 4. 2005; CD003723. Zohair Al Aseri MD,FRCPC EM & CCM
Status Epilepticus Treatment Benzodiazepines Study of out-of-hospital treatment of seizures lorazepamvsdiazepam. • Seizure activity terminated in • 60% of the lorazepam-treated patients • 43% of diazepam-treated patients • 21% of patients who received placebo Alldredge B.K., Gelb A.M., Isaacs S.M., et al: A comparison of lorazepam, diazepam, and placebo for the treatment of out-of-hospital status epilepticus. N Engl J Med 345. (9): 631-637.2001; Zohair Al Aseri MD,FRCPC EM & CCM
Status Epilepticus Treatment Benzodiazepines • When IV is not available alternative routes must be considered. • Both diazepam and lorazepam can be given rectally Appleton R., Sweeney A., Choonara I., et al: Lorazepam versus diazepam in the acute treatment of epileptic seizures and status epilepticus. Dev Med Child Neurol 37. (8): 682-688.1995; Chamberlain J.M., Altieri M.A., Futterman C., et al: A prospective, randomized study comparing intramuscular midazolam with intravenous diazepam for the treatment of seizures in children. Pediatr Emerg Care 13. (2): 92-94.1997; Towne A.R., DeLorenzo R.J.: Use of intramuscular midazolam for status epilepticus. J Emerg Med 17. (2): 323-328.1999; Zohair Al Aseri MD,FRCPC EM & CCM
IM midazolam outperformed IV lorazepam, with 73% of seizures terminating prior to arrival in the ED compared to 63% (p < 0.001). Zohair Al Aseri MD,FRCPC EM & CCM
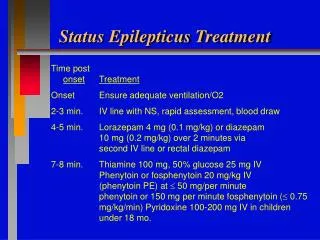
Status Epilepticus Treatment long history but weak evidence Phenytoin Dose: 20 mg/kg in a nonglucose solution, with a second dose of 10 mg/kg given if needed Target level: 15–20 mg/L. Zohair Al Aseri MD,FRCPC EM & CCM
Status Epilepticus Treatment • Limitations • Rate limited to 50 mg/min (25 mg/min in the elderly and patients with cardiovascular disease) • Hypotension, due to the propylene glycol diluent. • QT prolongation, cardiac monitoring is recommended • Extravasation can be disastrous extensive necrosis, namely the “purple glove syndrome.” need large IV Browne T.R.: The pharmacokinetics of agents used to treat statusepilepticus. Neurology 40. (5 Suppl 2): 28-32.1990; Zohair Al Aseri MD,FRCPC EM & CCM
Status Epilepticus Treatment Fosphenytoin • A prodrug of phenytoin • Has phosphoryl group, makes it water soluble with lower pH • Solution pH is 8.6–9. • Can be infused faster than phenytoin • Hypotension can stillrarely occur. Rosenow F., Arzimanoglou A., Baulac M.: Recent developments in treatment of status epilepticus: a review. Epileptic Disord 4. (Suppl 2): S41-S51.2002; Zohair Al Aseri MD,FRCPC EM & CCM
Status Epilepticus Treatment Fosphenytoin • Lower pH • decreases vascular irritation • decreases tissue toxicity • allowing for IM administration. • The conversion half-life is 8 to 15 minutes. • Measured in phenytoin equivalents (PE) and can be given at up to 150 mg PE/min. • No controlled studies of its use in SE. Browne T.R., Kugler A.R., Eldon M.A.: Pharmacology and pharmacokinetics of fosphenytoin. Neurology 46. (6 Suppl 1): S3-S7.1996; Zohair Al Aseri MD,FRCPC EM & CCM
Status Epilepticus Treatment Fosphenytoin Prepared as 500 PE/10 mL, that is, an intramuscular loading dose of 1000 PE would be a 20-mL injection. Fischer J.H., Patel T.V., Fischer P.A.: Fosphenytoin: clinical pharmacokinetics and comparative advantages in the acute treatment of seizures. Clin Pharmacokinet 42. (1): 33-58.2003; • Rapid achievement of therapeutic levels within 1 hour • Can be safely given in the buttocks • Need nursing protocols Zohair Al Aseri MD,FRCPC EM & CCM
Other First-Line Therapies: Valproate and Phenobarbital Valproate • Excellent safety profile. • Loading dose of 15 to 20 mg/kg in dextrose-containing solutions at a rate of 3 to 6 mg/kg/min. • Target levels: 75–100 mg/L Zohair Al Aseri MD,FRCPC EM & CCM
Other First-Line Therapies: Valproate and Phenobarbital Retrospective 63 patients overall efficacy of 63.3% and favorable tolerance of rapid administration. Valproate Limdi, N.; Shimpi, A.; Faught, E.; Gomez, C.; Burneo, J. Efficacy of rapid IV administration of valproic acid for status epilepticus. Neurology 2005, 64, 353–355. Zohair Al Aseri MD,FRCPC EM & CCM
Other First-Line Therapies: Valproate and Phenobarbital Valproate 68 pts two groups to study the efficacy of sodium valproate (VPA) and phenytoin (PHT). Seizures were aborted in 66% in the VPA 42% in the PHT group. As a second choice in refractory patients, VPA was effective in 79% and PHT was effective in 25%. Side effects in the two groups did not differ. Sodium valproate may be preferred in convulsive SE because of its higher efficacy. Misra, U.; Kalita, J.; Patel, R. Sodium valproate vs phenytoin in status epilepticus: A pilot study. Neurology 2006, 67, 340–342. Zohair Al Aseri MD,FRCPC EM & CCM
Other First-Line Therapies: Valproate and Phenobarbital • Small studies • Further study is needed. • Useful? in cases • Benzodiazepine use is limited by hypotension • Hypersensitivity to phenytoin Valproate in SE Zohair Al Aseri MD,FRCPC EM & CCM
Other First-Line Therapies: Valproate and Phenobarbital • It works on (GABAA) receptor, similar to benzodiazepines. Phenobarbital Shaner D.M et al: Treatment of status epilepticus: a prospective comparison of diazepam and phenytoin versus phenobarb and optional phenytoin. Neurology 38.(2):202-207.1988; One study demonstrated its equal to the combination of diazepam and phenytoin in the control of SE. Zohair Al Aseri MD,FRCPC EM & CCM
Other First-Line Therapies: Valproate and Phenobarbital Phenobarbital Problems • Profound respiratory depression and hypotension from its vasodilatory and cardiodepressant effects. • long half-life, which can make complications difficult to manage. Sillanpaa M., Shinnar S.: Status epilepticus in a population-based cohort with childhood-onset epilepsy in Finland. Ann Neurol 52. (3): 303-310.2002; Zohair Al Aseri MD,FRCPC EM & CCM
Other First-Line Therapies: Levetiracetam • Retrospectively • 32 patients treated with LEV i.v. for SE. • Benzoplus i.v. LEV terminated SE in 23 patients. • LEV could not terminate SE in seven patients. • Nausea and emesis in one. • Elevation of liver enzymes in one. Berning, S.; Boesebeck, F.; van Baalen, A.; Kellinghaus, C. Intravenous levetiracetam as treatment for status epilepticus. J. Neurol. 2009, 256, 1634–1642. Zohair Al Aseri MD,FRCPC EM & CCM
Billington, M.; Kandalaft, O.R.; Aisiku, I.P. Adult Status Epilepticus: A Review of the Prehospital and Emergency Department Management. J. Clin. Med. 2016, 5, 74. Zohair Al Aseri MD,FRCPC EM & CCM
Refractory Status Epilepticus • Current literature supports the use of continuous IV infusion of anesthetic doses of • midazolam • barbiturate • propofol • Inhalational anesthetics do not have a well-defined role Walker I.A., Slovis C.M.: Lidocaine in the treatment of status epilepticus. Acad Emerg Med 4. (9): 918-922.1997; Pascual J., Sedano M.J., Polo J.M., et al: Intravenous lidocaine for status epilepticus. Epilepsia 29. (5): 584-589.1988; Lampl Y., Eshel Y., Gilad R., et al: Chloral hydrate in intractable status epilepticus. Ann Emerg Med 19. (6): 674-676.1990; Yeoman P., Hutchinson A., Byrne A., et al: Etomidate infusions for the control of refractory status epilepticus. Intensive Care Med 15. (4): 255-259.1989; Zohair Al Aseri MD,FRCPC EM & CCM
Therapy for Refractory Status Epilepticus Midazolam • Midazolam preferred for continuous infusion in because of its short duration • A loading dose of 0.2 mg/kg is followed by an infusion of 0.05 to 2.0 mg/kg/h. Kumar A., Bleck T.P.: Intravenous midazolam for the treatment of refractory status epilepticus. Crit Care Med 20. (4): 483-488.1992; Zohair Al Aseri MD,FRCPC EM & CCM
Therapy for Refractory Status Epilepticus Propofol • Another GABAA agonist • Limited studies in refractory SE • There is evidence that it provides almost immediate suppression of seizure activity after a bolus infusion. • Rapid recovery • 3 to 5 mg/kg followed by infusion at 1 to 15 mg/kg/h. Be aware of propofol infusion syndrome Brown L.A., Levin G.M.: Role of propofol in refractory status epilepticus. Ann Pharmacother 32. (10): 1053-1059.1998; Zohair Al Aseri MD,FRCPC EM & CCM
Therapy for Refractory Status Epilepticus Anesthetic Barbiturates • Pentobarbital and thiopental are much shorter acting than phenobarbital. • Both agents are highly lipid soluble and will accumulate in fat stores, leading to prolonged elimination. Zohair Al Aseri MD,FRCPC EM & CCM
Therapy for Refractory Status Epilepticus Anesthetic Barbiturates • Thiopental more lipid soluble and the metabolic pathway can become saturated, • leading to an accumulation of thiopental and delays in recovery when stopped. • Pentobarbital is preferred when a barbiturate is used to manage refractory status. • Load with 5 to 15 mg/kg over 1 hour. • Infusion can be started at 0.5 to 10.0 mg/kg/h. Hypotension is an issue in both Vignatelli L., Tonon C., D’Alessandro R.: Incidence and short-term prognosis of statusepilepticus in adults in Bologna, Italy. Epilepsia 44. (7): 964-968.2003; Manno E.M.: New management strategies in the treatment of statusepilepticus. Mayo Clin Proc 78. (4): 508-518.2003; Zohair Al Aseri MD,FRCPC EM & CCM
Yasiry Z, Shorvon SD. The relative effectiveness of five antiepileptic drugs in treatment of benzodiazepine-resistant convulsive status epilepticus: a meta-analysis of published studies. Seizure 2014;23:167-74 • avoid phenobarbital where the risk of hypotension or respiratory depression are significant • avoid valproate where there is a particular susceptibility to hyperammonaemia or hepatic failure (possibly in children with mental handicap) Zohair Al Aseri MD,FRCPC EM & CCM
Yasiry Z, Shorvon SD. The relative effectiveness of five antiepileptic drugs in treatment of benzodiazepine-resistant convulsive status epilepticus: a meta-analysis of published studies. Seizure 2014;23:167-74 Conclusion • Valproate, levetiracetam and phenobarbital can all be used as first line therapy in benzodiazepine-resistant status epilepticus. The evidence does not support the first-line use of phenytoin. There is not enough evidence to support the routine use of lacosamide. Randomized controlled trials are urgently needed. Zohair Al Aseri MD,FRCPC EM & CCM
Which Anticonvulsants Are Efficacious as Initial and Subsequent Therapy? Efficacious at stopping seizures lasting at least 5 minutes (level A). With IV access IV lorazepam IVdiazepam (with or without phenytoin) IM midazolam IV phenobarbital = = = > IV lorazepam IV phenytoin IV lorazepam Without IV access IM midazolam >
Which Anticonvulsants Are Efficacious as Initial and Subsequent Therapy? After failure of a benzodiazepine (level C). • IV valproic acid = IV phenytoin =continuous IV diazepam as 2nd therapy • No data exist about the efficacy of levetiracetam (keppra) as either initial or second therapy.
What Adverse Events Are Associated With Anticonvulsant Administration? • Respiratory and cardiac symptoms are the most common encountered adverse events with IV anticonvulsant • No substantial difference exists between anticonvulsants in regard to cardiorespiratory adverse event • Placebo has higher rate of cardiorespiratory complications.
Future study for SE The Established Status Epilepticus Treatment Trial (ESETT) Currently enrolling patients Comparing (valproate, phenytoin, and levetiracetam) Zohair Al Aseri MD,FRCPC EM & CCM
If still seizing with benzo, 2nd line anticonvulsant and sedation?? Think about autoimmune seizure Zohair Al Aseri MD,FRCPC EM & CCM
Status Epilepticus Morbidity related to • Cerebral hypoxia • Direct neuronal death • Systemic effects such as: • Hypoxia • Hypoperfusion • Metabolic acidosis • Hyperthermia • Rhabdomyolysis • Hypoglycemia Zohair Al Aseri MD,FRCPC EM & CCM