Download
1 / 50
580 likes | 978 Views
Status Epilepticus. by Robert S. Fisher, M.D., Ph.D. Department of Neurology Stanford, California USA. Definition of Status Epilepticus. A state of continuing seizures for greater than 30 minutes, or recurrent seizures for at least 30 minutes without intervening

E N D
Status Epilepticus by Robert S. Fisher, M.D., Ph.D. Department of Neurology Stanford, California USA
Definition of Status Epilepticus A state of continuing seizures for greater than 30 minutes, or recurrent seizures for at least 30 minutes without intervening return of consciousness.
TYPES OF STATUS Simple partial motor Complex partial Absence Myoclonic Tonic-clonic Epilepsia partialis cont. Non-convulsive Tonic-clonic * * Petit mal, spike-wave, absence
About 30,000 per year Rochester Richmond
Walton & Treiman Epilepsia 1995 S4:45 The longer you wait, the harder to treat 5 4 3 2nd sz mg Valium 2 1st sz 1 0 With delay of treatment, more diazepam is required to stop seizures in an experimental model of status.
% SURVIVING 110 EARLY TREATMENT IS KEY rapid treatment 100 90 <1hr >1hr 80 70 delayed treatment 60 0 5 10 15 20 25 30 35 DAYS DeLorenzo, 1992 Epilepsia S4:15
Epilepsy Status Symptomatic 2,000,000 140,000 60,000 Idiopathic
CONCEPT OF - Overt status - Subtle status • Encephalopathy • Mild twitching • Unresponsiveness • EEG general ictal
Cerebrovascular CAUSES OF STATUS: ADULTS Med change Anoxia ETOH-drug Metabolic Unknown Fever/infection Trauma Tumor % Congenital 0 5 10 15 20 25 30 from DeLorenzo et al. Epilepsia 1992; 33 (Suppl. 4): S15-25
COMPLICATIONS OF STATUS Hyperthermia Shock Rhabdomyolysis Arrhythmias Aspiration Physical Injuries Psychosocial Brain cell loss Death in 5-30% Iatrogenic injury
MISDIAGNOSIS • Walker MC, Howard RS, Smith SJ, Miller DH, • Shorvon SD, Hirsch NP. Diagnosis and treatment • of status epilepticus on a neurological intensive • care unit. QJM 1996; 89: 913-20. • 26 pts admitted to neuro-ICU as status epilepticus • Only 14 (54%) were in status epilepticus • Six were in drug-induced coma or were encephalopathic • Six had pseudo-status epilepticus: 4 were intubated.
SEQUENCE OF EEG CHANGES IN STATUS EPILEPTICUS • Discrete seizures • Waxing ictal • Continuous ictal • Continuous ictal with flat • PLEDs on flat background
100 µV 1 sec FP1-F7 Discrete seizures F7-T3 T3-T5 T5-O1 FP2-F8 F8-T4 T4-T6 T6-O2
Continuous ictal discharges FP1-F7 F7-T3 T3-T5 T5-O1 FP2-F8 F8-T4 T4-T6 T6-O2 200 µV 1 sec
PLEDS Fp1-F7 F7-T3 T3-T5 T5-O1 Fp2-F8 F8-T4 T4-T6 T6-O2 Fp1-F3 F3-C3 C3-P3 P3-O1 Fp2-F4 F4-C4 C4-P4 P4-O2 100 µV 1 sec
STAGE OF EEG & RESPONSE TO THERAPY 80 70 % recovery 60 50 % 40 30 20 10 0 Discrete Waxing Continuous Cont with flat PLEDs Treiman et al. from VA study 1996
In 1685, King Charles II of England suffered from an illness that caused him to have convulsions. The treatments he underwent included: "letting" of one pint of blood; an enema of antimony, sacred bitters, rock salt, marrow leaves, violets, beetroot, chamomile flowers, fennel seeds, linseed, cinnamon, cardamon seeds, and aloe; and having his head shaved and blistered. Needless to say, the King died. quoted in: http://www.epilepsynl.com/newsletters/NewsletterFall2004.pdf Charles II of England King of Scots, King of England and King of Ireland (and Ruler of the American Colony) Reign: 29 May 1660 – 6 February 1685 Born: 29 May 1630 Died: 6 February 1685
HOW NOT TO TREAT STATUS A 42 year old male known alcohol abuser was brought to the ER stiff and trembling. He was thought to be exhibiting DT's (1), and was there- fore given diazepam by NG tube. This precipitated emesis and associated aspiration (2). Then all 4 extremities began to jerk rhythmically.
HOW NOT TO TREAT STATUS An iv was established, and routine bloods sent to the lab (3). Anticonvul- sants were withheld for 45 minutes pending arrival of the medical record (4). Seizure activity was terminated with 10 mg diazepam iv push, but tonic-clonic movements recurred 15 minutes later (5). Phenytoin 300 mg was given intra- muscularly to no effect (6).
HOW NOT TO TREAT STATUS Phenobarbital 500 mg iv was given as a third drug, resulting in apnea and hypo- tension (7). The patient resided in an ICU for 24 hours, whereupon he awoke, exhibited no further seizures, and was discharged that day (8)
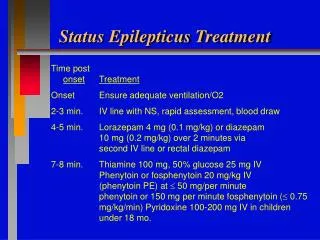
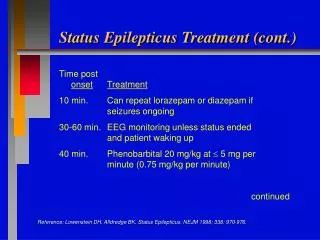
PRINCIPLES FOR STATUS 1. Secure the correct diagnosis 2. Stabilize patient first 3. Treat the treatable 4. Stop within 30 minutes 5. Immediate + long-term control 6. Proper routes and doses of meds 7. Expect cardiorespiratory trouble 8. Diagnosis and follow-up
STABILIZE • Airway • Breathing • Circulation • Oxygen • Dextrose ?
MONITOR • Breathing • Pulse • Blood Pressure • EKG • EEG
VA COOP STATUS STUDY Ten Centers, 530 evaluable patients Four iv regimens for initial Rx GTC status PHT 18 mg/kg DZP 0.15 mg/kg, then PHT 18 mg/kg PBB 15 mg/kg LOR 0.1 mg/kg Endpoint: seizure-free from 20-60 minutes Clinical EEG Treiman et al. from VA study 1996
CONTROL BY DRUG 70 60 50 40 % 30 20 10 0 LOR PBB DZP+PHT PHT
You stop the visible seizures, but the patient doesn’t wake up for an hour. What should you do?
Treiman et al. from VA study 1996 20% had EEG status continuing after behavioral seizures had stopped. 80% 20%
No differences among four treatment group for : Rate of recurrence 39 day outcome Adverse events Treiman et al. from VA study 1996
Outcome Overt Subtle Improved, discharged 53% 9% Still in hospital 21% 25% Died 27% 65% Treiman et al. 1996 VA Coop But – is usual outcome really this poor?
Shneker BF, Fountain NB. Assessment of acute morbidity and mortality in nonconvulsive status epilepticus. Neurology 2003;61:1066-1073. • 100 consecutive ICU NCSE patients. • 18 (18%) died: 14/52 (27%) in acute medical group 1/31 (3%) in the epilepsy group 3/17 (18%) in the cryptogenic group • Mental status impairment was severe in 33 • Complications occurred in 39
DRUG THERAPY • lorazepam (Ativan) • phenytoin (Dilantin) • phenobarbital • pentobarbital • propofol (Diprivan) • midazolam (Versed) • isofluorane • etomidate • lidocaine • paraldehyde • magnesium • furosemide • cooling ???
CVP line or Swan • Load: 5-15 mg/kg in 250 cc NS over 1 hr • Orders for neosynephrine or pressors • Continuous EEG monitoring • Maintain 1-20 mg/kg per minute • Aim for about 70-90% EEG suppression • Taper after a few days over half a day PENTOBARBITAL
100 µV 1 sec FP1-F7 F7-T3 T3-T5 T5-O1 FP2-F8 F8-T4 T4-T6 T6-O2 FP1-F3 F3-C3 C3-P3 P3-O1 FP2-F4 F4-C4 C4-P4 P4-O2
Quicker wake-up Maybe less respiratory depression Bolus of 2 mg/kg Continuous infusion 1-10 mg/kg/hr (17-170 ug/kg/m) EEG monitoring with titration to burst-suppression Supportive care for comatose patients Be aware of expense PROPOFOL: USE IN STATUS
PROPOFOL: ADVERSE EFFECTS Respiratory depression with induction > 2.5 mg/kg Hypotension in about 15% Bradycardia in about 5% < 0.2% of 25,981 pts needed hemodynamic support Increases serum triglycerides Lipid, egg, glycerol solvent may get infected Propofol infusion syndrome (rare) Sometimes paradoxical induction of seizures
Triphasics vs. Nonconvulsive Status • Difficult EEG distinction, perhaps impossible • Both show periodic frontal 3-phase sharp potentials • Triphasics can have an after-going slow wave • Both wax and wane • Both can have an anterior-posterior gradient • Triphasics tend to decline with sleep (but variably) • Waxing-waning awareness in both • Involves BDZ receptors in both • What is metabolic encephalopathy anyway?
FP1-F7 F7-T3 T3-T5 T5-O1 FP2-F8 F8-T4 T4-T6 T6-O2 FP1-F3 F3-C3 C3-P3 P3-O1 FP2-F4 F4-C4 C4-P4 P4-O2 100 µV 1 sec Triphasic waves
SPECIAL CIRCUMSTANCES • Need IV medication • phenytoin • fosphenytoin • phenobarbital • diazepam, lorazepam, midazolam • Depacon (valproic acid) • paraldehyde (if obtainable) • levetiracetam (Keppra) • lacosamide (Vimpat)
SPECIAL CIRCUMSTANCES Need to avoid sedation Most except phenobarbital benzodiazepines
SPECIAL CIRCUMSTANCES Need to avoid WBC depression Most OK, Except carbamazepine oxcarbazepine valproic acid felbamate
SPECIAL CIRCUMSTANCES Need to avoid low sodium Most OK, Except carbamazepine oxcarbazepine
COMMON MISTAKES • Fail to recognize status • Fail to deliver emergency support • Not treating reversible causes • Hypoglycemia • Hypocalcemia • Hypoxia • Toxic ingestion • Hyperthermia • Other reversible causes • Too slow with meds • Partial polypharmacy
CONCLUSIONS • Status is common and lethal • Early/effective treatment makes a difference • Subtle status can be missed • First support the patient & treat the treatable • Lorazepam is the favored therapy • Several other drugs can be used later: e.g., • propofol or pentobarbital coma • 7. With best therapy, mortality remains high