Download
1 / 1
70 likes | 318 Views
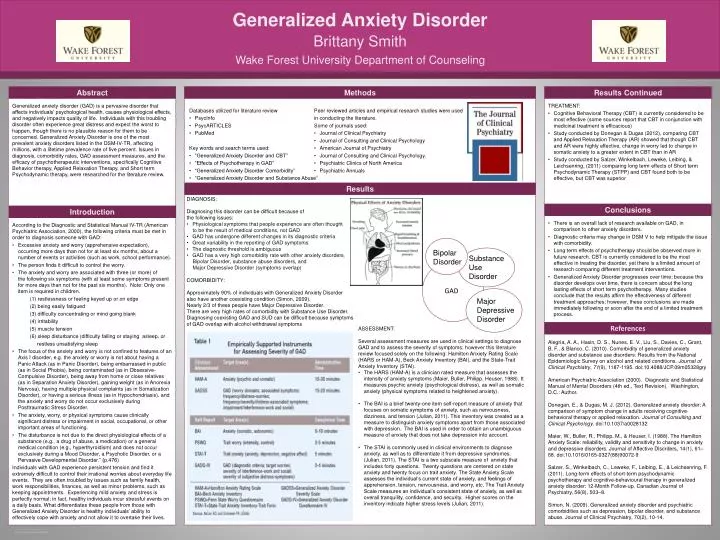
Generalized Anxiety Disorder. TREATMENT: Cognitive Behavioral Therapy (CBT) is currently considered to be most effective (some sources report that CBT in conjunction with medicinal treatment is efficacious)

E N D
Generalized Anxiety Disorder TREATMENT: Cognitive Behavioral Therapy (CBT) is currently considered to be most effective (some sources report that CBT in conjunction with medicinal treatment is efficacious) Study conducted by Donegan& Dugas (2012), comparing CBT and Applied Relaxation Therapy (AR) showed that though CBT and AR were highly effective, change in worry led to change in somatic anxiety to a greater extent in CBT than in AR Study conducted by Salzer, Winkelbach, Leweke, Leibing, & Leichsenring, (2011) comparing long term effects of Short term Psychodynamic Therapy (STPP) and CBT found both to be effective, but CBT was superior Generalized anxiety disorder (GAD) is a pervasive disorder that affects individuals’ psychological health, causes physiological effects, and negatively impacts quality of life. Individuals with this troubling disorder often experience great distress and expect the worst to happen, though there is no plausible reason for them to be concerned. Generalized Anxiety Disorder is one of the most prevalent anxiety disorders listed in the DSM-IV-TR, affecting millions, with a lifetime prevalence rate of five percent. Issues in diagnosis, comorbidity rates, GAD assessment measures, and the efficacy of psychotherapeutic interventions, specifically Cognitive Behavior therapy, Applied Relaxation Therapy, and Short term Psychodynamic therapy, were researched for the literature review. Abstract Methods Results Results Continued Introduction Conclusions There is an overall lack of research available on GAD, in comparison to other anxiety disorders. Diagnostic criteria may change in DSM V to help mitigate the issue with comorbidity. Long term effects of psychotherapy should be observed more in future research. CBT is currently considered to be the most effective in treating the disorder, yet there is a limited amount of research comparing different treatment interventions. Generalized Anxiety Disorder progresses over time; because this disorder develops over time, there is concern about the long lasting effects of short term psychotherapy. Many studies conclude that the results affirm the effectiveness of different treatment approaches; however, these conclusions are made immediately following or soon after the end of a limited treatment process. References According to the Diagnostic and Statistical Manual IV-TR (American Psychiatric Association, 2000), the following criteria must be met in order to diagnosis someone with GAD: Excessive anxiety and worry (apprehensive expectation), occurring more days than not for at least six months, about a number of events or activities (such as work, school performance). The person finds it difficult to control the worry. The anxiety and worry are associated with three (or more) of the following six symptoms (with at least some symptoms present for more days than not for the past six months). Note: Only one item is required in children. (1) restlessness or feeling keyed up or on edge (2) being easily fatigued (3) difficulty concentrating or mind going blank (4) irritability (5) muscle tension (6) sleep disturbance (difficulty falling or staying asleep, or restless unsatisfying sleep The focus of the anxiety and worry is not confined to features of an Axis I disorder, e.g. the anxiety or worry is not about having a Panic Attack (as in Panic Disorder), being embarrassed in public (as in Social Phobia), being contaminated (as in Obsessive-Compulsive Disorder), being away from home or close relatives (as in Separation Anxiety Disorder), gaining weight (as in Anorexia Nervosa), having multiple physical complaints (as in Somatization Disorder), or having a serious illness (as in Hypochondriasis), and the anxiety and worry do not occur exclusively during Posttraumatic Stress Disorder. The anxiety, worry, or physical symptoms cause clinically significant distress or impairment in social, occupational, or other important areas of functioning. The disturbance is not due to the direct physiological effects of a substance (e.g., a drug of abuse, a medication) or a general medical condition (e.g., hyperthyroidism) and does not occur exclusively during a Mood Disorder, a Psychotic Disorder, or a Pervasive Developmental Disorder.” (p.476) Individuals with GAD experience persistent tension and find it extremely difficult to control their irrational worries about everyday life events. They are often troubled by issues such as family health, work responsibilities, finances, as well as minor problems, such as keeping appointments. Experiencing mild anxiety and stress is perfectly normal; in fact, healthy individuals incur stressful events on a daily basis. What differentiates these people from those with Generalized Anxiety Disorder is healthy individuals’ ability to effectively cope with anxiety and not allow it to overtake their lives. Wake Forest University Department of Counseling Brittany Smith Alegría, A. A., Hasin, D. S., Nunes, E. V., Liu, S., Davies, C., Grant, B. F., & Blanco, C. (2010). Comorbidity of generalized anxiety disorder and substance use disorders: Results from the National Epidemiologic Survey on alcohol and related conditions. Journal of Clinical Psychiatry, 71(9), 1187-1195. doi:10.4088/JCP.09m05328gry American Psychiatric Association (2000). Diagnostic and Statistical Manual of Mental Disorders (4th ed., Text Revision). Washington, D.C.: Author. Donegan, E., & Dugas, M. J. (2012). Generalized anxiety disorder: A comparison of symptom change in adults receiving cognitive-behavioral therapy or applied relaxation. Journal of Consulting and Clinical Psychology. doi:10.1037/a0028132 Maier, W., Buller, R., Philipp, M., & Heuser, I. (1988). The Hamilton Anxiety Scale: reliability, validity and sensitivity to change in anxiety and depressive disorders. Journal of Affective Disorders, 14(1), 61–68. doi:10.1016/0165-0327(88)90072-9 Salzer, S., Winkelbach, C., Leweke, F., Leibing, E., & Leichsenring, F. (2011). Long-term effects of short-term psychodynamic psychotherapy and cognitive-behavioural therapy in generalized anxiety disorder: 12-Month Follow-up. Canadian Journal of Psychiatry, 56(8), 503–8. Simon, N. (2009). Generalized anxiety disorder and psychiatric comorbidities such as depression, bipolar disorder, and substance abuse. Journal of Clinical Psychiatry, 70(2), 10-14. • Databases utilized for literature review • PsycInfo • PsycARTICLES • PubMed • Key words and search terms used: • “Generalized Anxiety Disorder and CBT” • “Effects of Psychotherapy in GAD” • “Generalized Anxiety Disorder Comorbidity” • “Generalized Anxiety Disorder and Substance Abuse” • Peer reviewed articles and empirical research studies were used • in conducting the literature. • Some of journals used: • Journal of Clinical Psychiatry • Journal of Consulting and Clinical Psychology • American Journal of Psychiatry • Journal of Consulting and Clinical Psychology. • Psychiatric Clinics of North America • Psychiatric Annuals • DIAGNOSIS: • Diagnosing this disorder can be difficult because of • the following issues: • Physiological symptoms that people experience are often thought • to be the result of medical conditions, not GAD • GAD has undergone different changes in its diagnostic criteria • Great variability in the reporting of GAD symptoms • The diagnostic threshold is ambiguous • GAD has a very high comorbidity rate with other anxiety disorders, • Bipolar Disorder, substance abuse disorders, and • Major Depressive Disorder (symptoms overlap) • COMORBIDITY: • Approximately 90% of individuals with Generalized Anxiety Disorder • also have another coexisting condition (Simon, 2009). • Nearly 2/3 of these people have Major Depressive Disorder. • There are very high rates of comorbidity with Substance Use Disorder. • Diagnosing coexisting GAD and SUD can be difficult because symptoms • of GAD overlap with alcohol withdrawal symptoms Bipolar Disorder Substance Use Disorder GAD Major Depressive Disorder • ASSESSMENT: • Several assessment measures are used in clinical settings to diagnose GAD and to assess the severity of symptoms; however this literature review focused solely on the following: Hamilton Anxiety Rating Scale (HARS or HAM-A), Beck Anxiety Inventory (BAI), and the State-Trait Anxiety Inventory (STAI). • The HARS (HAM-A) is a clinician rated measure that assesses the intensity of anxiety symptoms (Maier, Buller, Philipp, Heuser, 1988). It measures psychic anxiety (psychological distress), as well as somatic anxiety (physical symptoms related to heightened anxiety). • The BAI is a brief twenty-one item self-report measure of anxiety that focuses on somatic symptoms of anxiety, such as nervousness, dizziness, and tension (Julian, 2011). This inventory was created as a measure to distinguish anxiety symptoms apart from those associated with depression. The BAI is used in order to obtain an unambiguous measure of anxiety that does not take depression into account. • The STAI is commonly used in clinical environments to diagnose anxiety, as well as to differentiate it from depressive syndromes. • (Julian, 2011). The STAI is a two subscale measure of anxiety that includes forty questions. Twenty questions are centered on state anxiety and twenty focus on trait anxiety. The State Anxiety Scale assesses the individual’s current state of anxiety, and feelings of apprehension, tension, nervousness, and worry, etc. The Trait Anxiety Scale measures an individual’s consistent state of anxiety, as well as overall tranquility, confidence, and security. Higher scores on the inventory indicate higher stress levels (Julian, 2011).