Download
1 / 7
80 likes | 395 Views
TRANSRADIAL ROTABLATION OF A CASE OF CTO. Dr. Christian Pristipino Coronary Intervention Unit San Filippo Neri Hospital Rome, Italy. Clinical Features. 76 years old man Severe, treated, hypertension Type IIb Dyslipidemia Severe Parkinson disease (bradikinesia and tremor)

E N D
TRANSRADIAL ROTABLATION OF A CASE OF CTO Dr. Christian PristipinoCoronary Intervention UnitSan Filippo Neri HospitalRome, Italy
Clinical Features • 76 years old man • Severe, treated, hypertension • Type IIb Dyslipidemia • Severe Parkinson disease (bradikinesia and tremor) • Sick sinus syndrome with previous pacemaker implant • Anterior myocardial infarction 6 months prior the procedure • Antero-lateral ischemia and anterior myocardial viability at stress/reperfusion thallium scintigraphy
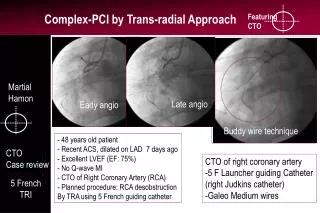
Technical Details • Left transradial approach with 6 Fr radial sheath (Cordis) • 6 Fr. XB 3.5 guiding catheter. Wiring D1 (BMW 0,014”, Guidant) followed by direct stenting (Medtronic AVE S7 3 x 15 mm @ 12 atm) • Crossing LAD occlusion with Guidant Cross-it 200 guidewire but failure to cross the lesion with balloon 1,5 mm (Aqua, Cordis) • Replacement of 6 Fr. transradial sheath with 7 Fr. femoral sheath positioned in left radial artery • Deep seating with 7 Fr. XB 3.5 guiding catheter. Crossing LAD occlusion with extrabackup guidewire, rotablation with 1,25 mm. bur (Boston Scientific), final stenting (Cordis Cypher 3 x 33 mm @ 12 atm) • Total procedure time: 60 min.; fluo time: 11 min; X ray exposition: 232 cGy
D1 Procedure 2.Wiring and direct D1 stenting D1 Occluded LAD 3. Final result on D1
LAD Procedure 5. Stenting LAD 4. Wiring and Rotablating LAD 6. Final result
Follow-up at 1 year Initial picture 1 yearresult D1 D1 Occluded LAD LAD • Patient remained asymptomatic at 1 year • LVEF improved from 39% to 48%, NYHA class improved from 2 to 1
Final remarks • Desocclusion of calcified CTOs is a complex procedure requiring rotablation in selected cases • Rotablation can be performed by transradial approach, even for CTOs, but require an even stronger backup than for less complex lesions • A major backup can be obtained also by transradial approach with Guiding catheters >= 7 Fr. deeply seated in coronary ostia • Transradial rotablation performed by experienced operators in complex cases can be well tolerated even when patient condition are critical, such as in parkinson disease with severe tremor.