Download
1 / 1
10 likes | 109 Views
Repetitive Transcranial Magnetic Stimulation May Benefit Motor Recovery After Incomplete Spinal Cord Injury: A Case Study Foreman, J., Masel, B. MD Transitional Learning Center • Galveston, Texas. Background

E N D
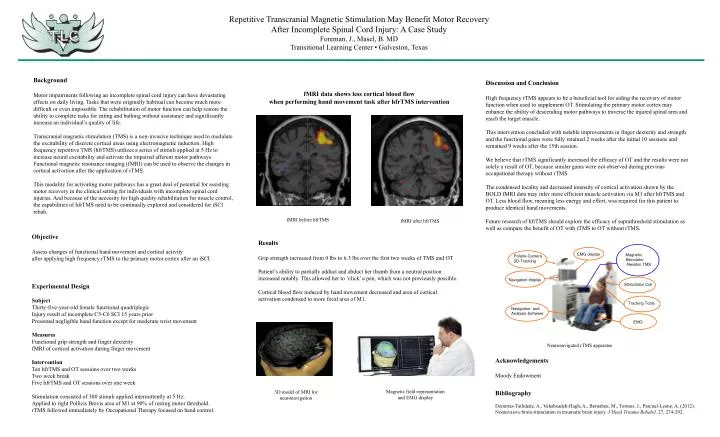
Repetitive Transcranial Magnetic Stimulation May Benefit Motor Recovery After Incomplete Spinal Cord Injury: A Case StudyForeman, J., Masel, B. MDTransitional Learning Center • Galveston, Texas Background Motor impairments following an incomplete spinal cord injury can have devastating effects on daily living. Tasks that were originally habitual can become much more difficult or even impossible. The rehabilitation of motor function can help restore the ability to complete tasks for eating and bathing without assistance and significantly increase an individual’s quality of life. Transcranial magnetic stimulation (TMS) is a non-invasive technique used to modulate the excitability of discrete cortical areas using electromagnetic induction. High frequency repetitive TMS (hfrTMS) utilizes a series of stimuli applied at 5 Hz to increase neural excitability and activate the impaired afferent motor pathways. Functional magnetic resonance imaging (fMRI) can be used to observe the changes in cortical activation after the application of rTMS. This modality for activating motor pathways has a great deal of potential for assisting motor recovery in the clinical setting for individuals with incomplete spinal cord injuries. And because of the necessity for high quality rehabilitation for muscle control, the capabilities of hfrTMS need to be continually explored and considered for iSCI rehab. Discussion and Conclusion High frequency rTMS appears to be a beneficial tool for aiding the recovery of motor function when used to supplement OT. Stimulating the primary motor cortex may enhance the ability of descending motor pathways to traverse the injured spinal area and reach the target muscle. This intervention concluded with notable improvements in finger dexterity and strength and the functional gains were fully retained 2 weeks after the initial 10 sessions and remained 9 weeks after the 15th session. We believe that rTMS significantly increased the efficacy of OT and the results were not solely a result of OT, because similar gains were not observed during previous occupational therapy without rTMS. The condensed locality and decreased intensity of cortical activation shown by the BOLD fMRI data may infer more efficient muscle activation via M1 after hfrTMS and OT. Less blood flow, meaning less energy and effort, was required for this patient to produce identical hand movements. Future research of hfrTMS should explore the efficacy of suprathreshold stimulation as well as compare the benefit of OT with rTMS to OT without rTMS. fMRI data shows less cortical blood flow when performing hand movement task after hfrTMS intervention fMRI before hfrTMS fMRI after hfrTMS Objective Assess changes of functional hand movement and cortical activity after applying high frequency rTMS to the primary motor cortex after an iSCI Experimental Design Subject Thirty-five-year-old female functional quadriplegic Injury result of incomplete C5-C6 SCI 15 years prior Presented negligible hand function except for moderate wrist movement Measures Functional grip strength and finger dexterity fMRI of cortical activation during finger movement Intervention Ten hfrTMS and OT sessions over two weeks Two week break Five hfrTMS and OT sessions over one week Stimulation consisted of 300 stimuli applied intermittently at 5 Hz. Applied to right Pollicis Brevis area of M1 at 90% of resting motor threshold. rTMS followed immediately by Occupational Therapy focused on hand control. Results Grip strength increased from 0 lbs to 6.3 lbs over the first two weeks of TMS and OT Patient’s ability to partially adduct and abduct her thumb from a neutral position increased notably. This allowed her to ‘click’ a pen, which was not previously possible. Cortical blood flow induced by hand movement decreased and area of cortical activation condensed to more focal area of M1. Neuronavigated rTMS apparatus Acknowledgements Moody Endowment Bibliography Demirtas-Tatlidede, A., Vahabzadeh-Hagh, A., Bernabeu, M., Tormos, J., Pascual-Leone, A. (2012). Noninvasive brain stimulation in traumatic brain injury. J Head Trauma Rehabil. 27, 274-292. Magnetic field representation and EMG display 3D model of MRI for neuronavigation






















