Download
1 / 16
170 likes | 575 Views
Epstein Barr Virus in Immunosuppressed Host. Epstein Barr Virus. = Human herpesvirus 4 Infects more than 95% of the world's population. Humans are the only known reservoir of Epstein-Barr virus. EBV is present in oropharyngeal secretions and is most commonly transmitted through saliva.

E N D
Epstein Barr Virus • = Human herpesvirus 4 • Infects more than 95% of the world's population. • Humans are the only known reservoir of Epstein-Barr virus. • EBV is present in oropharyngeal secretions and is most commonly transmitted through saliva. • The virus replicates in nasopharyngeal epithelial cells. • Viral replication viremia lymphoreticular system, including the liver, spleen, and B lymphocytes in peripheral blood. • Host immune response to the viral infection includes activation of CD8+ T lymphocytes • = atypical lymphocytes found in the peripheral blood. • The T lymphocytes kill EBV-infected B cells and eventually reduce the number of Epstein-Barr virus–infected B lymphocytes to less than 1 per 106 circulating B cells. • Latent viral infection of memory B cells
Clinical Manifestations • Most commonly associated with infectious mononucleosis • Classically affects adolescents and young adults • Children often asymptomatic • Self-limited course • Classic triad of symptoms
Sore throat +/- tonsillar Exudate (85% of pts) Lymphadenopathy (usually posterior cervical chain) Present in ~100% of pts
Fever! – 98% of pts ** e.g. Saturday Night Fever
Rash! • Generalized maculopapular, urticarial or petechial rash • Erythema nodosum has been reported, but is rare • Rash more common in pts treated with antibiotics (esp. ampicillin or amoxicillin)
Reactive Lymphocytes! • Lymphocytosis = most common lab finding • Absolute count > 4500 • Differential count > 50% • Most pt’s have >10% atypical lymphocytes on peripheral smear • = CD8+ Tcells
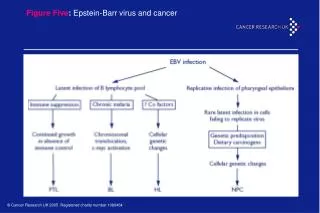
Less common manifestations of EBV “EBV can affect virtually any organ.” • Hepatitis Fulminant liver failure • Jaundice is rare • Glomerulonephritis/ Acute Kidney Injury • Pneumonia/Pleural effusion • Myocarditis • Pancreatitis • Myositis
Hepatitis! Increased infiltration by CD8+ T cells Inflammation of the liver Transaminitis
Neurologic syndromes • Guillian-Barre • Cranial nerve palsies • Encephalitis • Aseptic meningitis • Transverse myelitis • Optic neuritis
Oral Hairy Leukoplakia! Vs. Oral Candidiasis
Epstein-Barr virus serology • Antibodies to Epstein-Barr virus antigens • Antibodies to viral capsid antigen (VCA), • early antigens (EAs) • Epstein-Barr nuclear antigen (EBNA). • Primary acute Epstein-Barr virus infection is associated with VCA-IgM, VCA-IgG, and absent EBNA antibodies. • The antibody pattern in recent infection (3-12 mo) includes positive findings for VCA-IgG and EBNA antibodies, negative VCA-IgM antibodies, and, usually, positive EA antibodies. • Patients who are immunocompromised and have persistent or reactivated Epstein-Barr virus infections often have high levels of antibodies to EA/D or EA/R.
Monospot • Rapid slide agglutination tests, including Monospot assays, have been developed to measure acute infectious mononucleosis heterophile antibodies in a rapid qualitative fashion. Slide tests use either horse RBCs or bovine RBCs. • All commercial kits for rapid diagnosis of acute infectious mononucleosis heterophile antibodies have low sensitivity (63-84%), with a negative predictive value of more than 10%. • Spot tests rarely yield false-positive results in patients with lymphoma or hepatitis.
Treatment • In most cases, no treatment is necessary ---------------------------------------------------- • Corticosteroids for tonsillar edema / respiratory distress • In vitro trials of acyclovir • Our patient was treated with Valcyte 900mg po q day • IVIG for immune-mediated thrombocytopenia

![Epstein Barr Virus [EBV] - Named after Epstein and Barr](https://cdn5.slideserve.com/9727845/epstein-barr-virus-ebv-named-after-epstein-dt.jpg)