Download
1 / 17
210 likes | 610 Views
INFECTIOUS MONONUCLEOSIS ( epstein-barr virus). Professor: Ma lian. Typical features. Prolong fever Exudative pharyngitis Generalized adenopathy Hepatosplenomegaly Atypical lymphocytes Heterophil antibodies. General considerations.

E N D
INFECTIOUS MONONUCLEOSIS(epstein-barr virus) Professor: Ma lian
Typical features • Prolong fever • Exudative pharyngitis • Generalized adenopathy • Hepatosplenomegaly • Atypical lymphocytes • Heterophil antibodies
General considerations • Infectious mononucleosis (mono) is a common acute infectious disease usually found in individuals between the ages of 5 and 30. • Pathogeny • Epstein-Barr virus (90%) • CMV, HIV, HHV-6, toxoplasma gondii, Hepatitis virus etc (5-10%).
EBV • Occur worldwide • Transmitted by saliva and blood transfusion • Related with the following diseases • Mono • Burkitt lymphoma • Nasopharyngeal cancer
Clinical findings • Symptoms and signs • Prolong fever(>39℃) • Soft palate petechiae and Exudative pharyngitis • Generalized adenopathy • Splenomegaly and hepatomegaly • Rash (macular,scarlatiniform or urticarial) • eye edema • X-linked lymphoproliferative syndrome (XLP): occur in the children with primary immunodeficiency disease
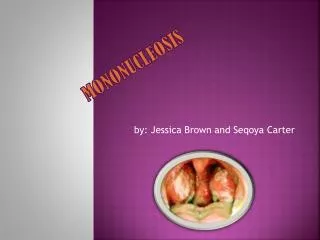
Sore throat Soft palate petechiae Exudative pharyngitis
Generalized adenopathy usually in the neck,armpit, and throat
Clinical findings • Laboratory findings • Peripheral blood • Atypical lymphocytes • Leukopenia • Heterophil antibodies • Anti-EBV antibodies • aminotransferase
No clumping of the red bloods cells indicates the person's serum does not contains heterophile antibodies. The few clumps that are seen are red blood cells from the test reagent that did not separate during shaking of the reagent prior to placing it on the slide. Clumping of the red bloods cells indicates the person's serum contains heterophile antibodies.
Differantial diagnosis • Group A streptococcal infection • Rubella • Adenovirus • Hepatitis A or B • Toxoplasmosis • Drug reaction • Leukemia • CMV mononucleosis • HIV infection
Complication • CardiorespiratoryInterstitial pneumonitisMyocarditisPericarditisPleuritis • HematologicAutoimmune hemolytic anemiaImmune granulocytopenia or thrombocytopeniaPancytopenia
Complication • HepaticCholestatic jaundice (severe hepatitis)Massive hepatic necrosis and failure • NeurologicCranial nerve palsiesGuillain-Barré syndromeMeningoencephalitisTransverse myelitisOthers
Infectious mononucleosis hepatitis Marked mononuclear cell infiltration of the sinusoids without significant necrosis. H&E stain. Infectious mononucleosis heapatitis High power of previous illustration showing the signs of high regenerative activity: binucleate cells and a mitotic figure. H&E stain.
Treatment • No specific therapy exists for IM, but general support helps • rest and fluids • acetaminophen or aspirin for fever and aches; • lozenges, salt-water gargles, • viscous lidocaine hydrochloride for sore throat.
Treament • Acyclovir, ganciclovir, and foscarnet • IVIG • α-interferon • Antibiotics and corticosteroids are indicated only for complications. • Patients with splenomegaly should advoid sport for 6-8 weeks.