Download
1 / 27
270 likes | 353 Views
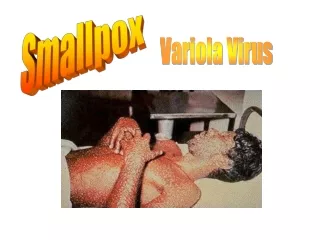
Smallpox Virus . Case 16. Nadine Rodriguez Mary Uy Diana Perez. Unreported Outbreak!. Summer of 1971 in Aralsk (Soviet republic of Kazakhstan July 15, 1971 Biological research vessel called the Lev Berg set sail from Aralsk on an extended voyage

E N D
Smallpox Virus Case 16 Nadine Rodriguez Mary Uy Diana Perez
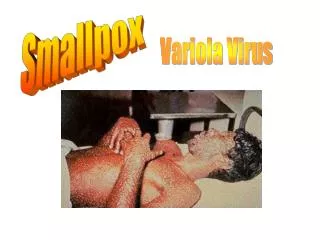
Unreported Outbreak! • Summer of 1971 in Aralsk (Soviet republic of Kazakhstan • July 15, 1971 • Biological research vessel called the Lev Berg set sail from Aralsk on an extended voyage • Ship strayed inadvertenly near the Vozrozhdeniye Island • Biological weapons field testing site by Soviet Ministry of Defense • Released 400 grams of weaponized smallpox within 15 kilometers of the island
Patient 1 • After arriving home in Aralsk on August 12 • Patient 1- Fever, headache, and muscle aches (vaccinated) • Local doctor visit: • Noted fever of 39°C and a cough. • Prescribed antibiotics and aspirin • No definitive diagnosis • Shortly thereafter, diffuse rash covered her entire body and her fever broke • Everyone in her family including herself has been vaccinated against smallpox http://www.nlm.nih.gov/medlineplus/smallpox.html
Patient 2, Brother of Patient 1 • August 27, 15 days later… • Patient 2- Nine year old boy (vaccinated) • Fever and rash • Pediatrician diagnosed • Hives • Treated with tetracycline • Recovered over the next two weeks
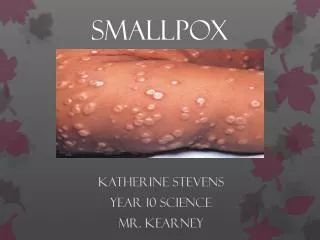
Patient 2 • Classic for smallpox • Very high temperature. • Followed by a pustular rash which covered his whole body • Pustules about 2 – 3 mm in diamter • Rash lasted 2 weeks and then crusted over • Smallpox scars from the rash disappeared over a 2 yr. time period www.zkea.com
More Patients! • Next three weeks • Physicians in Aralsk saw eight additional patients • Six adults and two children • Two children unvaccinated against smallpox • Developed hemorrhagic complications and died • One adult died from hemorrhagic variant of the disease www.visualsunlimited.com
Classification • Family: Poxviridae • Sub family: Chordopoxvirinae (vertebrates) • Two Species of Variola Vera: • Variola Minor • Variola Major • Double stranded linear DNA genome • Core plus 2 lateral bodies and a lipoprotein coat and an envelope • Larger than other viruses
Smallpox Endemic Areas 1945 Endemic smallpox http://www.bt.cdc.gov/agent/smallpox/training/overview/
Endemic Importations Transmission Interrupted Smallpox Endemic Areas 1967 http://www.bt.cdc.gov/agent/smallpox/training/overview/
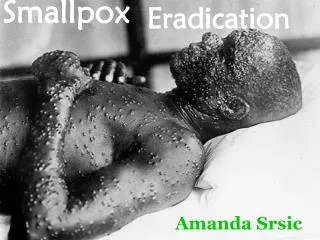
Only human infectious disease to have been completely eradicated in nature. Eradication 1979: Why and How ? Devastating Outcomes: Longterm – skin scars from lesions Occasional – blindness due to corneal ulcerations, and infertility in men. Possible Death A very contagious disease that is unique to humans, NO other known carriers Smallpox Virus http://en.wikipedia.org/wiki/Smallpox http:www.globalsecurity.org/wmd/library/report/1997/cwbw
Smallpox Declared Eradicated! • Only human infectious disease to have been completely eradicated in nature. • Has not been contracted naturally since 1977. • Declared eradicated by W.H.O. 1979.
How it is spread (Epidemiology) • Two main routes of entry: • Air droplets make contact with lungs (most common) • Face to face contact- especially sneezing/ coughing. • Inhalation of Aerosolized virus or virus droplets, can include circulation through ventilation system. • Direct contact with virulent rash or bodily fluids • Kissing, touching (without protective gear). • Sexual intercourse/ other forms of exchanging blood and body fluids • Contact with Fomites (less effective)- Bedding, blankets, clothing of infected persons. http://www.rhodes.edu/biology/glindquester/viruses/pagespass/smallpox/smallpox.html
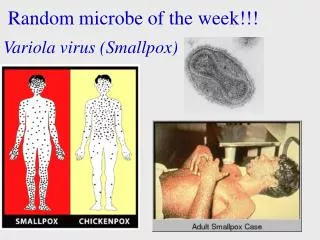
Diagnosis: Smallpox vs. Chickenpox • Despite some clinical similarities Smallpox can be easily distinguished from Chickenpox. • Chickenpox localizes on the covered areas of the body. • Smallpox localizes on uncovered areas of the body. • Chickenpox lesions are easy to pop, while smallpox lesions are harder to touch and more difficult to pop. • Chickenpox have varied growth stage, and smallpox have same growth stage http://www.scq.ubc.ca/?p=426
Timeline -Day 1-12 Incubation-no symptoms, feel fine, not contagious. -Day 12-14 Pre-eruption/prodromal stage-sudden onset high fever, malaise, headache, backache. Sometimes: respiratory distress, sneezing, coughing, abdominal pain and vomiting. -Day 14-17 Vesicular rash begins to form-2-3” diameter vesicles. Also, temperature decreases, and patient begins to feel a little better. blindness due to corneal ulcerations and infertility in men. Patient now contagious! -Day 20-32 Scabbing-Later scabs separate and fall off. Patients is contagious until last scab separates, patient is left with depressed depigmented scars. 1. http://www.zkea.com/archives/archive02001.html; 2. http://www.who.int/mediacentre/factsheets/smallpox/en/; 3. Donald Henderson et al. JAMA June 1999; 281:2127-37
Variola Minor vs. Variola Major • Mortality rate depends on variant type, case type, and vaccination status. Infection does not discriminate (sex, age,or race). • Higher probability of complications for pregnant women. • Variola Minor - causes a milder, less virulent form of the disease (alastrim) has a mortality rate of ~1% • Variola Major- mortality rate varies (30%-96%+). • Case types: Ordinary (Discrete/Confluent); Malignant/Flat; Hemorrhagic (of particular concern for use as Biological Weapon). http:www.globalsecurity.org/wmd/library/report/1997/cwbw http://www.bt.cdc.gov/agent/smallpox/training/overview/
Variola Major: Case Types - Differences in strain virulence and host response are responsible for varied clinical case types. • Ordinary (75-90% of Cases): 1. Discrete (Most common type) - refers to vesicles that have areas of normal skin between them 2. Confluent and Semi Confluent- blisters merge together into sheets. • Modified- Common in vaccinated individuals. • Less severe, lesions more superficial, not as infectious. • Fatality rate ~3% http://www.bt.cdc.gov/agent/smallpox/training/overview/ http:www.globalsecurity.org/wmd/library/report/1997/cwbw Semi-confluent
Variola Major: Case Types • Flat/Malignant (rare: ~2-5% of cases)- Rash/pustules appear flattened more superficial, and evolve slower. • Pustules ~4-5 mm diameter • Course of disease is similar to a burn, probably due to huge loss of skin by peeling. • Intense skin edema, abdominal pain, vomiting, mucosal/submucosal hemorrhage, tachycardia, infection/sepsis is a possible complication. • Mortification and death (70% mortality)- from tissue destruction. equivalent to third degree burns. http://www.bt.cdc.gov/agent/smallpox/training/overview/
Variola Major: Case Types • Hemorrhagic (rare: ~3% of cases)- Widespread • hemorrhage: under skin, eyes, organs. • Inflammatory Shock- Patients with high levels of circulating virus develop hemorrhagic complications as a result of host induced massive inflammatory response (non-specific immune response causes cloud of inflammatory mediators). • Can be confused for meningococcemia (severe blood infection caused by aggressive bacteria). May develop superficial purpuric papules. Doesn’t look like classic smallpox • Cause of death: hemorrhaging/blood loss; sepsis/toxemia can occur before rash even develops (Hyper-acute course). 1. http://www.bt.cdc.gov/agent/smallpox/training/overview/ 2. http:www.globalsecurity.org/wmd/library/report/1997/cwbw 3. http://www.journals.uchicago.edu/cgi-bin/resolve?id=doi:10.1086/381976&erFrom=-7477654646648014944Guest
Mortality Rates http://en.wikipedia.org/wiki/Smallpox http://www.bt.cdc.gov/agent/smallpox/training/overview/
Natural Smallpox : Effective bioweapon • Facilitated Spanish conquest of the Americas (Carribean 1507, Mexico 1520, Peru 1524, and Brazil 1555 ) • Used as a biological weapon during the French and Indian Wars of 1754-1767 when British forces in North America distributed blankets that had been used by smallpox patients to Native Americans collaborating with the French." http://en.wikipedia.org/wiki/Smallpox
Potentially More Dangerous Than Any Other Bioweapon! • Has a history of being tested and probably manipulated for bioweapons possibilities for at least a couple decades. • Cheap and easy to make and administer to unsuspecting populations. • Highly contagious- need relatively small amount of virus to cause a epidemic outbreak. • 2 week incubation period makes it hard to track. • No proven curative treatment • Naturally high mortality rate, which would be augmented by several present day factors. Including- history of virus testing and manipulation, general population would have probably lost vaccination induced immunity by now (lasts up to ~20yrs), Increased levels of Immunodeficient populations (HIV/AIDS).
Potentially More Dangerous Than Any Other Bioweapon! 43% of the US population who are under 30 years old have never received vaccinations for smallpox If a terrorist were to release a small amount of the virus into the air, the virus could infect the population within 6 to 24 hours. But because of recent increase on global terrorist activity, the US has prepared enough vaccine to administer to the public
Spread of Disease Prevented In The Past Edward Jenner (1749-1823) - In the eighteenth century, Jenner hypothesized that milkmaids who were infected by cowpox were resistant to smallpox - Experimental procedure ∙ Injected a boy with the fluid of cowpox blister ∙ Once the boy recovered from cowpox, he was then injected with smallpox - Results ∙ Boy remained healthy despite inoculation http://www.vaclib.org/news/jenner.jpg
Preventative Measures & Treatments • Pre-exposure • Vaccinations • Made from another pox-type virus, vaccinia • 95% success rate • Post-exposure • Vaccinations • Within three days, can completely prevent or lesson the severity of symptoms • Four to seven days, vaccine offers limited protection modifying severity http://www.aapa.org/clinissues/images/vaccinia_vaccine.jpg
Treatment Once lesions appear No known cure Isolation 3-4 weeks, or until all scabs have fallen off Supportive therapy and antibiotics Supportive care Treatment for complications: Flat/malignant- treat as burn. Fluid/electrolyte/nutritional replacement. Debridement and topical antibiotic to prevent infection. Hemorrhagic- treat as septic shock- Oxygen/ to relieve respiratory distress (if present), fluids, treat low blood pressure, support any poorly functioning organs. Vaccination- prevention is the best medicine http://www.who.int/mediacentre/factsheets/smallpox/en/
Possible Treatments Currently Being Researched Cidofovir A DNA antiviral medication normally used to treat an infection known as cytomegalovirus (CMV). May work if giving within two days of exposure. Blockage of viral protein E3L binding site from DNA Researchers from MIT and Arizona State University Viral protein E3L binds to the DNA causing the infect. Hybrid antibodies National Institute of Allergy and Infectious Disease Composed of chimpanzees and human antibodies that blocks B5 protein
Works Cited • Henderson, D. A., Inglesby, T. V., Bartlett, J. G., & et al. Smallpox as a biological weapon medical and public health management. 1999.The Journal of American Medical Association 281 (22) 2127-2137. • Infectious disease smallpox treatment. 2007. Mayo Foundation for Medical Education and Research. <http://www.mayoclinic.com/health/smallpox/DS00424/DSECTION=6>. • Jenner, Edward. Advameg Inc. 2007. <http://www.discoveriesinmedicine.com/General-Information-and-Biographies/Jenner-Edward.html>. • http://www.who.int/mediacentre/factsheets/smallpox/en/ • http://www.aapa.org/clinissues/images/vaccinia_vaccine.jpg • http://www.vaclib.org/news/jenner.jpg • http://www.bt.cdc.gov/agent/smallpox/training/overview/ • http://www.nlm.nih.gov/medlineplus/smallpox.html • http://www.bt.cdc.gov/agent/smallpox/training/overview/ • http://en.wikipedia.org/wiki/Smallpox • http:www.globalsecurity.org/wmd/library/report/1997/cwbw • http://www.rhodes.edu/biology/glindquester/viruses/pagespass/smallpox/smallpox.html • http://www.scq.ubc.ca/?p=426 • http://www.zkea.com/archives/archive02001.html • http://www.who.int/mediacentre/factsheets/smallpox/en/