Download
1 / 102
1.19k likes | 1.91k Views
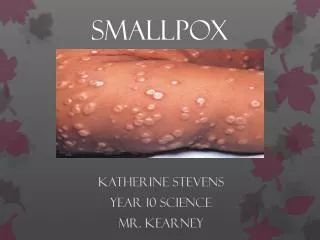
Smallpox. Charlotte McKinley Jessica Midence Izabella Messina. Smallpox. Smallpox is a serious, contagious and sometimes fatal disease. There is no specific treatment for smallpox, and the only prevention is vaccination.

E N D
Smallpox Charlotte McKinley Jessica Midence Izabella Messina
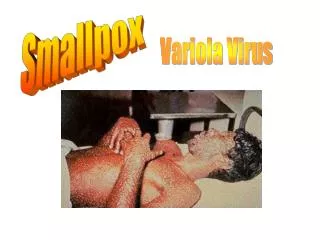
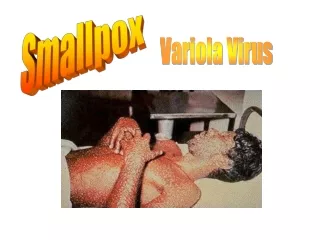
Smallpox • Smallpox is a serious, contagious and sometimes fatal disease. • There is no specific treatment for smallpox, and the only prevention is vaccination. • The name smallpox is derived from the latin word “spotted” and refers to the raised bumps that appear on the face and body of an infected person. • Smallpox is in the Orthopoxvirus genus of viruses.
Origin of Smallpox • The name Variola was first used in the 6th century. Derived from the Latin word varius (spotted) or varus (pimple). • Anglo-Saxons in the 10th century used the word poc or pocca (bag or pouch) to describe an exanthemous disease, possibly smallpox. • In the 15th century, the English used the prefix small to distinguish variola the smallpox from syphilis, the great pox.
First Case of Smallpox • There is no animal reservoir, and no human carriers. • First certain evidence comes from the mummified remains of Ramses. (1157 B.C.) • Written descriptions did not appear until the 10th century in Southwestern Asia.
Smallpox Travel • Smallpox was likely carried from Egyptian traders to India during the millennium B.C. where it became established as an endemic infection. • Epidemics of the disease can be found in the bible, and in ancient Greek and Roman literature. • From Asia and Africa smallpox spread with increasing frequency into less populous areas, and then into Europe.
Smallpox in the Ancient World • Peloponnesian Wars (430 B.C.) • Thucydides recorded smallpox symptoms. • A person aboard a ship from North Africa came to Athens infected with smallpox. • Described as violent heats, unnatural, putrid odors, stomach distress, and the body covered with small pustules and ulcers. • Also noted that those who survived became immune.
Smallpox in the New World • In the early 16th century smallpox began to imported into the western hemisphere. • The Spanish inadvertently owe success in conquering the Aztec and Incas in Mexico to smallpox. • Smallpox arrived in North America via Canada, and Mexico.
Smallpox as Biological Warfare • Lord Jeffrey Amherst, Commanding General of British Forces in North America during the French and Indian War. (1754-1763) • Used blankets (smallpox blankets) coated with smallpox dust as germ warfare to wipe out the Native American population.
History of Variolation and Vaccine • Known that survivors became immune to the disease. • As a result, physicians intentionally infected healthy persons with smallpox organisms. • Variolation is the act of taking samples (pus from pustules or ground scabs) from patients whose disease had been benign, and introducing it into others through the nose or skin.
Survival Rates with Variolation • Two to Three percent of variolated persons died of smallpox, became the source of a new epidemic, or developed other illnesses from the lymph of the donor such as tuberculosis or syphilis. • The case fatality rates were still ten times lower in those that were variolated compared to those with naturally occurring smallpox. • Side effects of variolation were the appearance of smallpox itself, but it would disappear after a week or so.
Variolation in the New World • Reached the New World in 1721. • Used to stop the epidemic in Boston. • In 1766 American Soldiers under George Washington were unable to take Quebec from the English because of smallpox. • Smallpox was apparently one of the main causes of the preservation of Canada in the British Empire. • In 1777 Washington had all of his soldiers variolated beginning with new military operations.
Cows, Milkmaids, and the Pox • In rural areas of Europe it was known the milkmaids became immune to smallpox after developing smallpox • 1774, farmer Benjamin Jesty was the first to vaccinate his wife and kids with material taken from the utters of cows. • 1791, school teacher Peter Plett vaccinated his students with material from the utters of cows.
Edward Jenner • Studied to become a physician in England. • In May of 1776 dairymaid Sarah Nelmes consulted Jenner about a rash on her hand. • He took this opportunity to test the protective properties of cowpox against smallpox. • Determined that cowpox can be passed from person to person as well as from cow to person. • The next step was to see if the cowpox would protect the patient from smallpox.
Edward Jenner • Jenner published the data collected in 1798. • However, Jenner’s technique did not catch on as anticipated. • After more and more people were becoming immune to smallpox vis a vis cowpox it became accepted as the way of the future. • In 1840 variolation was forbidden by an Act of Parliament. • In England vaccination with cowpox became compulsory in 1853.
Edward Jenner • Jenner spent his time supplying cowpox material to others around the world. • In recognition of his work the British government awarded Jenner ten thousand pounds in 1802, and twenty thousand pounds in 1807. • Jenner was honored for his technique, and vaccine became the universally used term to indicate introducing material under the skin to produce a protection against disease.
Eradication • In 1801 Jenner said, “The annihilation of the smallpox, the most dreadful scourge of the human species, must be the final result of this practice.” • Compulsory vaccinations began in the following years: • 1807 in Bavaria • 1810 in Denmark • 1835 in Prussia • 1853 in Britain
Eradication • Even after vaccination outbreaks still continued because the virus was imported by travelers where there were still endemics. • Not until after WWI did most of Europe become smallpox free, and not until after WWII was transmission stopped throughout Europe and North America. • In less developed countries smallpox continued largely unabated until the middle of the 20th century.
Eradication • 1940s: large scale preparations of a stable freeze dried vaccine was perfected by Collier. • 1950: Pan American Sanitary Organization decided to undertake a hemisphere wide eradication program. • 1958: Union of Soviet Socialist Republics proposed to the WHO that a global smallpox eradication program be undertaken.
Eradication • The campaign was based on a two fold strategy. • 1) Mass vaccination campaigns in each country using a vaccine of ensured potency and stability that would reach at least 80% of the population. • 2)Development of a system to detect and contain cases and outbreaks.
Eradication • 26 October 1977 the last naturally occurring case of smallpox was recorded in Merka Somalia. • In 1978 two cases were reported. These were both from people working in labs with smallpox in England.
Eradication • 1980: WHO formally declared that smallpox was dead. • The eradication of smallpox was one of the most important branches of modern medicine. • Jenner has been acknowledged as the father of immunology,
TAXONOMY • FAMILY: POXVIRIDAE • SUBFAMILY: CHORDOPOXVIRINAE (infect vertebrates) • GENERA: ORTHOPOXVIRUS (variola, vaccinia, cowpox, monkeypox) • AVIPOXVIRUS (fowlpox) • CAPRIPOXVIRUS (sheep-pox) • LEPORIPOXVIRUS (myxoma) • PARAPOXVIRUS (milker’s nodule) • SULPOXVIRUS (swinepox) • 2. SUBFAMILY: ENTOMOPOXVIRINAE (infect arthropods)
CHARACTERISTICS SHARED BY SPECIES OFORTHOPOXVIRUS : • - The largest and most complex viruses • Virons particles can be seen with a light microscope • - They contain a linear genome of a single • double-stranded DNA • They replicate in the cytoplasm of the host cell, • therefore they must provide their own mRNA and • DNA synthetic machinery • (including DNA-dependent RNA polymerase) • - Inclucison bodies: type B and type A • Virions have a brick-like shape and are present in • 2 forms, both are infectious: • 1. EEV (Extracellular Enveloped Virus) • 2. IMV (Intracellular Mature Virus) • Serological cross-reactivity • - Produce a hemagglutininin antigen (HA) • - Vaccinia is the most intensively studied member of • the poxvirus family
Fenner,F. et al. Smallpox and Its Eradiction. Genevea, Switzerland:WHO. 1998:1460
Fenner,F. et al. Smallpox and Its Eradiction. Genevea, Switzerland:WHO. 1998:1460
MORPHOLOGY OF THE VIRION - have an brick-like shape; dimensions 400x200nm - four major elements: 1. core ( 9 nm thick membrane, biconcave disk, a tightly compressed nucleoprotein) 2. lateral bodies ( unknown function) 3. outer membrane ( a protein shell 12nm thick, the surface consists of irregularly arranged tubules) 4. envelope ( an inconstant element, proteins are glycosylated and acylated) - Virons are present in two infectious forms: 1. EEV (Extracellular Enveloped Virus)- released from cells spontaneously, by exocytoses are enclosed within a lipoprotein envelope, which contains the haemagglutinin and other specific polypeptides - CEV (Cell Associated Enveloped Virus) 2. IMV (Intracellular Mature Virus) – released by cellular disruption, lacks envelope, “naked virus”
VacciniaVirus – Electron micrographs A. Non- enveloped virion (surface of outer membrane with tubular elements) C. Thin section of non-enveloped virion (biconcave core) B. Enveloped virion, found in extracellular medium D. Viral core, released after treatment of virions with Nonidet Fenner,F. et al. Smallpox and Its Eradiction. Genevea, Switzerland:WHO. 1998:1460
VIRAL REPLICATION – CELL CYCLE Fenner,F. et al. Smallpox and Its Eradiction. Genevea, Switzerland:WHO. 1998:1460
VIRAL REPLICATION – CELL CYCLE http://www.rkm.com.au/VIRUS/SMALLPOX/smallpox-life-cycle.html
CELLULAR CHANGES “Viral factory” visualized in stained cells as the B-type inclusion body, is first seen at 2.5h cupules first appear at 4 hours and some are completed as immature particles 6-8hours. From 8 hours onwards mature particles appear. “Toxic”changes may occur in the inf.cells, which in monolayer cultures become rounded and retract from each other. Fenner,F. et al. Smallpox and Its Eradiction. Genevea, Switzerland:WHO. 1998:1460
Cytoplasmic inclusion bodies in infected cells B-type (Guarnieri bodies)- sites of viral replication produced by all orhopoxviruses A-type – strongly eosinophilic, found in cells infected with: cowpox,ectromelia and raccoonpox virus; appear late in the infection and are not associated with viral replication (may contain mature virions) Fenner,F. et al. Smallpox and Its Eradiction. Genevea, Switzerland:WHO. 1998:1460
STRUCTURE OF THE VIRAL GENOME - Contains a single linear molecule of a double stranded DNA About 200 kbp long; guanine+cytosine content 36% - when denatured the two sister strands form a large single-stranded circular molecule, being attached at each end of the genome by covalent links - for the most part, the DNA sequences in the central part of the genome are unique, but the terminal fragments (inverted terminal repeats) cross-hybridize with each other and with the termini of other species of orthopoxvirus - Schemat of vaccinia virus DNA - The ITR’s include: an A+T-rich, incompletely base-paired, hairpin loop that connects the two DNA strands; set of short tandemly repeated sequences. The ITR’s are variable in length owing to deletions, repetitions, and transpositions - Inverted repeats in vaccinia are 10 kbp long in variola are 725 bp - Variola vs. Vaccinia: genomes are highly conserved with >95% nucleotide identity, however towards the termini the sequences diverge Poxviruses that have been inactivated that don’t damage their DNA can be reactivated
VIRAL PROTEINS • Encodes about 200 proteins • The central part of the genome encodes for structural and functional proteins; • Virulence genes are found near the inverted repeats, • -numerous virus-encoded enzymes,are packaged within the virus core, • including: • * multisubunit DNA-dependent RNA polymerase • * RNA polymerase associated protein of 94kd (RAP94) • * a transcription factor (VETF) • * capping and methylating enzymes • * poly(A) polymerase • These components are used to synthesize translatable mRNA • -Importatnt proteins for replication: • * topoisomerase • * thymidine kinase – allows the incorporation of Thymidine into DNA • * thymidylate kinase – catalyzes the reversible phosphorylotransfer between ATP and TMP • * ribonuceoside reductase – converts ribonucleoside diphosphates ( NDP’s ) into deoxyNDP’s • * dUTPase – minimize the misincorporation of Uracil into DNA • * Uracil-DNA gylclosylase – removes the RNA base (Uracil) from DNA • * DNA ligase
non enzymatic-VIRAL PROTEINS • Membrane proteins: • A33R, A34R, A36R :*N-glycosylated, phosphorylated • * fromation of actin tail and microvilli, which facilitate • viral dissemination • A36R : required for kinesin recruitment and is involved in • microtubule-based motility of IEV’s • A56R: Hemagglutinin, N- and O- glycosylated , promote cell fusion and • cell to cell viral spread • A27L: required for the formation of IEV, fusion protein, • microtubule –dependent movment, • normal sized plaques , has additional role in the viral assembly • A28L: fusion protein; A28 deficient virions with normal amounts of A27 and • A17 (binding partner) are unable to induce cell fusion • 2. Core proteins: • F17R, L4R, A3L, A10L : account for ~70% of the viral core by weight, • bind DNA
VIRAL IMMUNOMODULATORY STRATEGIES • Poxviruses encode multiple classes of immunomodulatory proteins to inhibit • diverse processes as: • * apoptosis • * the production of interferon • * the production of chemokines and inflammatory cytokines • * the activity of complement, NK, CTL’s, antibodies 2. The inhibitory proteins, produced by virus, fall into three main classes: - Virokines * resemble host cytokines * secreted from infected cellsto block hosts receptors * vIL-10, vIL-18 - Viroreceptors * mimic host cellular receptors * altered cellular receptors that have lost their transmembrane sequnces and consequently are secreted from infected cells to sequester ligands * vINF-Rs, vTNFRs - Intracellular proteins * target host signal transduction pathways * inhibit inner antiviral pathways: apoptosis – vFLIP’s, serpins proinflammatory cascades - TNF
VIRAL IMMUNOMODULATORY PROTEINS j Johnston,J.B.et al.Poxvirus Immunomodulatory Strategis:Current Perspectives. Journal of Virology (2003), 77: p.6093-6100
VIRAL IMMUNOMODULATORY PROTEINS Complement Regulatory Proteins - VCP– Vaccinia virus Complement control Protein, consists of short consensus repeats found in hosts’ complement regulatory proteins. Inhibits the classic and alternative pathways of complement through binding and inactivating both C4b and C3b • SPICE- the smallpox inhibitor of complement enzymes • molecularly engineered homologue of VCP (Rosengrad et al;.Univ. of Penn.) • Demostrated: the functional advantage of variola complement regulatory protein • Over the vaccinia homologue • - More human complement specific than VCP • 100-fold more potent at inactivating C4b&C3b; • SPICE serves to inhibit the formation of the C3/C5 convertases necessary for • Complement-mediated viral clearance SPICE- provides the first evidence that variola proteins are particulary adept at overcoming human immunity, and the decreased function of VCP suggests one reason why the vaccinia virus vaccine was associated with relatively low mortality. Disabling SPICE may be useful therapeuticaly
Smallpox Clinical Presentations, Transmission, Treatment, Vaccination
Transmission of Smallpox • Humans are the only natural host of smallpox and it is not known to be transmitted by insects or animals (no animal reservoir) • Transmission generally occurs from direct and fairly prolonged face-to-face contact (in order for infected spit particles to pass from one person to another) • Infected aerosols and air droplets spread in face-to-face contact with an infected person after fever has begun, esp. if symptoms include coughing • Smallpox can also be spread through direct contact with infected bodily fluids or contaminated objects (ie. Bedding and clothing) • In rare instances, smallpox can spread through the air of an enclosed area • Variola major renders infected people bedridden so spreading to the community is reduced • In variola minor, however, the symptoms are so mild that patients remain ambulatory during the infection phase and can spread the virus more widely
Pathogenesis of Smallpox • The portal of entry for smallpox is the respiratory tract or inoculation on the skin • Excretions from the mouth and nose, rather than scabs, are the most important source of infectious virus • Studies have shown that primary infection in the nose or mouth do not produce a “primary lesion” that ulcerates and releases virions onto the surface • Four models have been studied to learn about the spread of the infection through the body: mousepox in mice, rabbitpox in rabbits, and monkeypox and smallpox in monkeys and apes • During incubation the virus proceeds through infection, replication, and liberation (usually accompanied by cell necrosis) first at the site of inoculation and then to the regional lymph nodes, then deeper lymph nodes and possibly into the bloodstream
Pathogenesis of Smallpox • When tests were performed on humans to determine the pathogenesis, the virus was only rarely collected from the serum of infected persons, even though viraemia had definitely occurred • Therefore it was determined that viraemia in ordinary smallpox was restricted to the pre-eruptive and early eruptive stages of the disease • In hemorrhagic smallpox, however, virus was readily found in the blood and titers were high; thus hemorrhagic smallpox can be associated with overwhelming infection and the continued release of virus into the bloodstream • The primary event for production of lesions of the rash in orthopoxvirus infections is localization (in the small blood vessels of the dermis) of virus particles that circulate in the bloodstream • Vasodilation leads to greater density of lesions
Pathogenesis of Smallpox • After introduction of smallpox into the oropharyngeal cavities it spreads to the regional lymph nodes • Asymptomatic viremia occurs on the 3rd or 4th day after infection, with further dissemination of the virus to spleen, bone marrow, and other lymph nodes. • The virus localizes in small blood vessels of the dermis and oropharyngeal mucosa, leading to initial onset of the enanthem and exanthem, at which point (about day 14) the patient becomes infectious • The spleen, lymph nodes, kidneys, liver, bone marrow, and other viscera also may contain large amounts of virus • Secondary viremia occurs by the 8th to 12th day after initial infection; this is followed by onset of fever and toxemia. • Smallpox is disseminated through the body in the lymph and bloodstream as cell-associated particles • Enveloped forms of the virus are more important than non-enveloped in the dissemination of the virions over a distance
Pathogenesis of Smallpox • The development and evolution of skin lesions is an extremely valuable clue to the diagnosis and involves the following steps: • Dilatation of the capillaries in the papillary layer of the dermis occurs initially, followed by swelling of the endothelial cells in the vessel walls; perivascular cuffing with lymphocytes, plasma cells, and macrophages can be seen. • Lesions then develop in the epidermis, where the cells become swollen and vacuolated; characteristic B-type inclusion bodies can be found in the cytoplasm. • The cells increase in size and the cell membranes rupture, leading to vesicular lesions. • Pustulation results from the migration of polymorphonuclear cells into the vesicle. • The contents of the pustule gradually become desiccated, leading to crusting or scabbing of the lesions. • Re-epithilialization and scarring occur as the lesions heal.
Effects on Other Organs • A striking feature of smallpox reports is that there is an absence of specific lesions anywhere except in the skin and mucous membranes • The endothelial cells lining the sinusoids of liver were often swollen and occasionally proliferating or necrotic (in more severe cases) • Reticulum cell hyperplasia occurred in bone marrow and spleen • Spleen was usually engorged with very numerous large lymphoid cells
Pathogenesis of Smallpox • When studies were done on rabbits with rabbitpox to determine the cause of death the rabbits had extreme hypertension, leading to a shock-like syndrome, decreased urinary output and a rise in blood-urea and plasma potassium levels • Death seemed to be caused by lethal concentrations of potassium ion, which was possibly from the hypertension
Clinical Presentations • Smallpox is also called Variola • 4 orthopoxviruses are known to infect humans: variola, vaccinia, cowpox, and monkeypox • Variola virus is strictly a human virus, although primates and other animals can be infected under lab conditions • Infection begins when the virus comes into contact with oropharyngeal (mouth and throat) or respiratory mucosa; virus multiplication then occurs in regional lymph nodes • There are 2 clinical forms of Smallpox: Variola Major and Variola Minor • Variola major is severe and the most common form with more extensive rash and higher fever with a death rate of about 30% • Variola minor has less common presentation and much less severe with death rate of 1% or less
Variola Major has 4 clinical presentations based on the nature and evolution of the lesions; those 4 types are: • Ordinary: most frequent (more than 90% of cases in both vaccinated and unvaccinated persons); corresponds to classical description of smallpox • Modified: milder and may occur in previously vaccinated people; rarely fatal • Flat and Hemorrhagic: very severe but uncommon