Download
1 / 35
411 likes | 580 Views
Slides prepared and compiled by highly experienced ENT teacher, Dr. Krishna Koirala from Nepal, for teaching undergraduate and postgraduate ENT students in the field of otorhinolaryngology. <br>A clear and concise explanation of the basic concepts in the subject matter concerned. <br>He is the Head of department with a sound knowledge in the field of ENT to teach both undergraduate and postgraduate ENT students<br>This presentation will be specially useful to all the students who are preparing for their MBBS ENT examination. This also will be a useful note for postgraduate ENT residents <br>

E N D
Diseases of the External ear Dr. Krishna Koirala
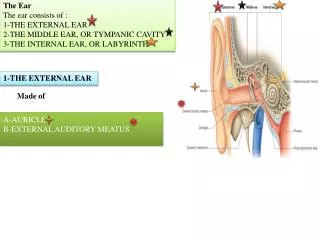
Congenital Minor: Accessory auricular tags , Bat ear Pre - auricular sinus Major : Anotia ,Microtia Traumatic Hematoma , lacerations Diseases of Pinna
3. Inflammatory : Perichondritis 4. Neoplastic : Squamous cell carcinoma Basal cell carcinoma 5. Others : Sebaceous cyst ,lipoma , keloids, Pseudocyst pinna
Preauricular sinus • Small pit leading to a blind tract that lies adjacent to helix • Due to incomplete fusion of first and second branchial arches (Hillocks of His) • Unilateral : L>R • Bilateral : (25 - 50%), more like to be hereditary • Mostly asymptomatic
Repeated infections • Surgical excision of the sinus with complete removal of tract along with a portion of auricular cartilage • Recurrence is common ( tracts arborize and follow a tortuous course)
Collection of blood and serum under the perichondrium of pinna Pathology : Shearing forces to the auricle and pinna resulting in separation of the perichondrium from the underlying cartilage Seen in boxers, wrestlers, judo players ,athletes More common on the lateral surface Pinna : Swollen, bluish, tender on touch Hematoma of the pinna
Infection • Perichondritis and abscess formation • Thickening and cauliflower ear • Necrosis of the cartilage • Treatment • Broad spectrum antibiotics sensitive to Pseudomonas and Staphylococcus. Eg. Ceftriaxone, ciprofloxacin • Wide bore needle aspiration and tight pressure dressing • Incision and drainage • Debridement of necrosed cartilage
Incision and drainage Vaseline gauze being applied Compression dressing on progress
Perichondritis • Inflammation of the perichondrium of auricular cartilage • Commonly caused by Pseudomonas • Predisposing factors • Laceration, piercing, mastoid surgery, otitis externa • Frostbite, burns, infections of pinna , relapsing polychondritis
Clinical Features • Pain & swelling of pinna • Tender pinna • Fluctuation +/- • Fever +/- • Treatment • High dose i.v. antibiotics eg. Ciprofloxacin , Ceftriaxone, Cefotaxime, Flucloxacillin, Amoxyclav, Cefuroxime • Local application of Magnesium sulphate • I & D of abscess • Surgical debridement to remove necrosed cartilage
Localized subperichondrial fluctuant swelling of the auricle Etiology : Idiopathic, Viral Frequently encountered during monsoon season Presence of sterile clear fluid in subperichondrial plane with no definite cyst wall Appears insidiously, mild discomfort + Variable size , fluctuation + Pseudocyst of pinna
Treatment Aspiration and quilting Surgical deroofing followed by buttoning Intralesional steroids following aspiration Incision and drainage with removal of a part of cartilage
Congenital Congenital atresia of EAC Stenosis Inflammatory Otitis externa Neoplastic Osteoma Squamous cell carcinoma Basal cell carcinoma Traumatic Iatrogenic / Accidental Miscellaneous Wax Foreign bodies Keratosis obturans Acquired atresia of EAC Exostoses Diseases of the External Auditory Canal
Otitis Externa Classification According to extent of lesion • Localized : Furunculosis • Diffuse : Idiopathic, Traumatic , Irritant, Allergic, Bacterial/ fungal, Climatic / environmental • Invasive : ( Granulomatous / Necrotizing / Malignant) • Part of generalized skin condition : Seborrhic dermatitis, Atopic, Allergic , Psoriasis • Others : Keratosis obturans
Furunculosis • Infection of hair follicle of external auditory canal by Staph. aureus , Pseudomonas • Painful, tender well circumscribed lesion • Pain aggravated by jaw movements • Meatus occluded by swelling – conductive hearing loss • Carbuncle / regional lymphadenitis • May coexist with diffuse otitis externa : otorrhea , debris • Postauricular swelling ( cellulitis / lymphadenopathy)
Treatment • Cleaning of EAC (Aural toileting) • Packing of EAC • Wick soaked in steroid antibiotic cream • Ichthamol Glycerin ( IG) : analgesic, anti inflammatory, antibiotic, dehydrator • Systemic antibiotics : Flucloxacillin, Ciprofloxacin • Analgesics • Warm saline dressings • Incision and drainage if suppuration occurs • Recurrence : R/O Diabetes mellitus !!!
Diffuse Otitis externa • Tropical ear/ Singapore ear • Aggravating factors : Local trauma , heat, humidity, bathing • Causative agents : Pseudomonas, Proteus, Staph. aureus • Stages • Acute • Earache aggravated by jaw movement • Swelling of the soft tissue around the ear • Red, swollen, tender canal skin • Pus / debris in the meatus • TM dull & injected
Chronic • Irritation of ear/discharge • Decreased hearing • Thickened meatus skin / reduced lumen with pus & debris • Granulations in the TM • Treatment • Careful cleaning of meatus preferably under the Microscope • Steroid - antibiotic ear packing or Antibiotic - steroid ear drops • Systemic antibiotics
Otomycosis • Fungal infection of EAC • Organisms : Aspergillus niger, Candida, Dermatophytes • Predisposing conditions : Extremely moist, hot environment, Chronic bacterial otitis externa • Symptoms : Itching , aural fullness, earache, discharge, swelling • Signs • Grayish white debris resembling wet filter paper filling the meatus ( Candida) • Black specks in the debris (conidiophores of Aspergillus) • Injected canal wall
Treatment • Thorough cleaning of all accumulated debris • Antiallergics, analgesics • Topical antifungals • Nystatin, clotrimazole (1%) for 2-3 wks • Topical gentian violet solution • Burrow's solution ( 5% aluminum acetate solution ) • Reduces the swelling and removes the debris
Malignant Otitis externa ( Skull base Osteomyelitis) • Rapidly progressive bacterial infection of external auditory meatus, surrounding soft tissues and skull base • Predisposing factors • Elderly , poorly controlled diabetics, atherosclerosis, immunosuppressed, prolonged steroid use, hypogama - globulinemia , AIDS
Causative organisms • Pseudomonas, Staph. epidermidis, Aspergillus fumigatus • Hallmark of disease • Granulation tissue at the junction of cartilaginous and bony EAC • Pain out of proportion of the disease in EAC
Spread of Disease Floor of MCF, Basisphenoid Thrombosis of lateral sinus, superior and inferior petrosal sinus Secondary osteomyelitis of petrous Apex IX, X, XI,XII cranial nerve palsy Parotid gland ,TMJ EAC Tympanic plate, Mastoid tip Tympanomastoid suture, Adjacent soft tissues Facial Palsy
Investigations • CBC, RBS / Urea • CT Scan / MRI • Gallium bone scan • Treatment • Control of diabetes and other predisposing factors • Debridement of necrotic tissues • Administration of antibiotics( high dose , broad spectrum) • Ciprofloxacin 750 mg twice daily for 6-12 weeks • Ceftriaxone 1 gm I.V. BD 7-10 Days
Keratosis obturans • Keratotic mass of desquamated epithelium in bony portion of EAC obstructing it • Pearly white / obscured by wax • Common age : 5 -20 yrs • Etiology • Idiopathic • Chronic hyperemia desquamation of keratin epidermal debris • Faulty migration of squamous epithelial cells • May be associated with bronchiectasis & sinusitis
Clinical Features • Pain in the ear, aural fullness • Bilateral symptoms in children • Unilateral predominately in adults • Hearing loss (conductive) , otorrhea (rare), tinnitus • Geometrically patterned keratin plug within the lumen of expanded ear canal( onion skin ) • Erosion and abnormal widening of deep osseous meatus(eburnated bony canal , ballooning of EAC) • TM usually intact • Mucopurrullent discharge (rare)
Treatment Removal of the Keratotic mass by instrumentation (LA /GA) Treatment of inflammation Keratolytics - not helpful Canalplasty ( recurrent cases) Regular follow – up , May recur!!