Download
1 / 19
190 likes | 332 Views
Predicting CAD in the CPU: ECG vs MIBI. (45 pts with suspected UA and non diagnostic ECG ). 96. 84. 79. 74. 74. 65. 35. 38. With chest pain. Without chest pain. Bilodeau et al, JACC 1991;1:1684-1691. Predicting events in the CPU: ECG vs MIBI. Varetto et al 1993.

E N D
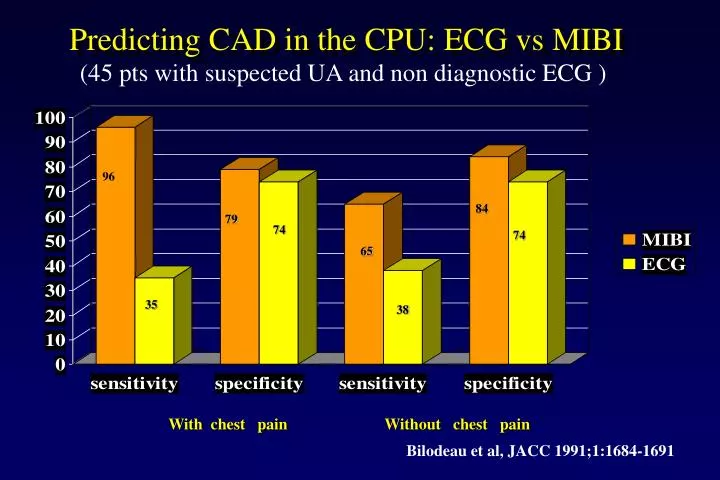
Predicting CAD in the CPU: ECG vs MIBI (45 pts with suspected UA and non diagnostic ECG ) 96 84 79 74 74 65 35 38 With chest pain Without chest pain Bilodeau et al, JACC 1991;1:1684-1691
Predicting events in the CPU: ECG vs MIBI Varetto et al 1993 Varetto et al, 1993
CLINICAL RISK CATEGORIES (ON RISK FACTORS AND ECG) Hilton et al, JACC 1994;23:1016-22
CARDIAC EVENTS AND RISK CATEGORIES IN THE ED P=0.0001 P=0.007 P=0.07 Hilton TC et al, JACC 1994;23:1016-22
CARDIAC EVENTS AND RISK CATEGORIES IN THE ED NS P<0.0001 P<0.0001 Hilton TC et al, JACC 1994;23:1016-22
SESTAMIBI SPECT AND OUTCOME Normal Abnormal Tatum et al, Ann Emerg Med 1997;29:116-125
PROGNOSTIC IMPACT OF Tc-99 TETROFOSMIN SPECT IMAGING IN THE ED 99 90 60 12 Heller et al, JACC 1998;31:1011-7
INCREMENTAL PROGNOSTIC VALUE OF TC-99 TETROFOSMIN SPECT IN THE ED 17,9 Incremental chi-square 7,8 5,5 A:age, gender B: A + >3 risk factors C: B + ecg, CP D: C + SPECT Heller et al, JACC 1998;31:1011-7
MYOCARDIAL SCINTIGRAPHY IN URGENCY (TRIAGE OF CHEST PAIN) NPV for AMI: > 99 % NPV (all events) :98 %
Troponin I as a Predictor of Major Cardiac Events in ED in Patients with Chest Pain Diagnostic performance of peak (1047 pts): > 0,4 ng/ml Diagnostic performance of first sample (808 pts) Polanczyk et al, JACC 1998; 32:8-14
Sensitivity of SestaMIBI and Troponin I Kontos et al, Circulation 1999; 99:2073-2078
EXERCISE TESTING IN Pts WITH CHEST PAIN SHORTLY AFTER PRESENTATION IN THE EMERGENCY Dpt Contraindications - ECG modifications - Enzyme rises - Persisting chest pain - Clinical indication to coronary arteriography Kirk JD et al. Ann Emerg. Med. 1998 Stein RA et al. Circulation 2000 Farkouh et al N. Engl. J. Med. 1999
EXERCISE TESTING IN Pts WITH CHEST PAIN SHORTLY AFTER PRESENTATION IN THE EMERGENCY Dpt Indications - 2 sets of enzymes at 4-h intervals normal - ECG at presentation and pre-exercise similar - Interpretable ECG, reliable for exercise testing - Patient must be asymptomatic or chest pain atypical In such Pts, exercise testing is safe, and a negative ETT selects a subgroup with less than 1% cardiac events in 6 months. In Pts with chest pain and a low-intermediate risk after clinical-lab-ECG triage, ETT in the CPU is highly cost-effective. Kirk JD et al. Ann Emerg. Med. 1998 Stein RA et al. Circulation 2000 Farkouh et al N. Engl. J. Med. 1999
Utility and safety of immediate exercise testing of low- risk patients admitted to the hospital with acute chest pain. - 190 non-consecutive low-risk patients admitted to the hospital from emergency department with acute chest pain. - ETT using Bruce protocol immediately on admission to the hospital (median time 165+30 min). - 111 (58.4%) negative exercise testing. - Among patients with negative ETT, during the 17+/-6 month follow-up only 8 (7.2%) experienced a cardiac event (1 AMI and 7angina). “...immediate ETT of low-risk patients with chest pain... is effective in further stratifying this group into those who can be safely discharged immediately…” Sarullo FM et al. Int J Cardiol 2000
Investigations on ETT in Chest Pain Units Tsakonis 1991 28 Pts 6 mo F-U No ETT events Kerns 1993 32 Pts 6 mo F-U No ETT events Gibler 1995 1010 Pts 30 d F-U No ETT events Gomes 1996 50 Pts No ETT events Zalenski 1998 317 Pts No ETT events Polanczyk 1998 276 Pts 6 mo F-U No ETT events Farkuoh 1998 424 Pts 6 mo F-U No ETT events NPP at follow-up: 98%. Highly cost-effective. Very safe.
“RULE OUT MYOCARDIAL INFARCTION” PROTOCOL (Brigham and Women’s Hospital Emergency Dpt)
“Although most admitted patients with chest pain (53%) were at low probability for AMI, only a minority (14%) were eligible for a short-stay protocol that required patients to be free of known coronary artery disease and able to perform an exercise tolerance test.” Zalenski RJ et al. Ann Emerg Med 1997
AHA Science Advisory Safety and Utility of Exercise Testing in Emergency Room Chest Pain Centers An Advisory From the Committee on Exercise, Rehabilitation, and Prevention, Council on Clinical Cardiology, AHA Circulation 2000; 102: 1463-7
SAFETY OF DOBUTAMINE STRESS ECHO IN THE CPUFOR THE EVALUATION OF COCAINE-ASSOCIATED CHEST PAIN (pilot study) - 24 patients with cocaine-associated chest pain - Normal ECG and troponin levels - No relevant side effects - 13/24 patients required supplement of atropine to reach their target heart rates. Dribben WH et al, Ann Emerg Med 2001.