Download
1 / 49
490 likes | 501 Views
Tubulointristitial Nephritis. Dr.boshra hasanzamani. Primary tubulointerstitial diseases Secondary tubulointerstitial disease. Primary tubulointerstitial diseases.

E N D
Tubulointristitial Nephritis Dr.boshra hasanzamani
Primary tubulointerstitial diseases Secondary tubulointerstitial disease
Primary tubulointerstitial diseases histologic and functional abnormalities that involve the tubules and interstitium to a greater degree than the glomeruli and renal vasculature.
Secondary tubulointerstitial disease occurs as a consequence of progressive glomerular or vascular injury.
Laboratory Manifestions • Acute rise in plasma creatinine concentration • Eosinophilia and eosinophiluria • Urine sediment: wbcs, rbcs, white cell casts • Proteinuria (< 1 g/day) • Signs of tubulointerstitial damage
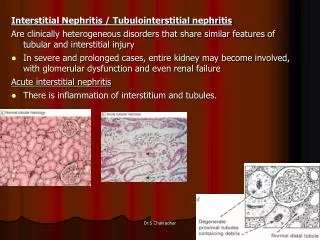
Interstitial Nephritis • Acute • Chronic
Acute Interstitial Nephritis interstitial edema cortical and medullary infiltration by both mononuclear cells and polymorphonuclear leukocytes patchy areas of tubule cell necrosis
Acute Interstitial Nephritis Therapeutic agents Infection Autoimmune Acute obstructive disorders
Therapeutic agents
Acute obstructive disorders
Clinical Features • classic presentation : - fever, rash, peripheral eosinophilia, and oliguric renal failure • occurring after 7–10 days of treatment with methicillin or another -lactam antibiotic
Atypical reactions : -nonsteroidal anti-inflammatory drug (NSAID)-induced AIN, in which fever, rash and eosinophilia are rare, but acute renal failure with heavy proteinuria is common
Diagnosis • unexplained renal failure with or without oliguria and exposure to a potentially offending agent • Peripheral blood eosinophilia adds supporting evidence • Urinalysis reveals pyuria with white blood cell casts and hematuria • Urinary eosinophils are neither sensitive nor specific for AIN • Renal biopsy is generally not required for diagnosis
Crystal Deposition Disorders and Obstructive Tubulopathies • in patients treated with : - sulfadiazine for toxoplasmosis -indinavir for HIV -intravenous acyclovir for severe herpesvirus infections • Oliguric acute renal failure, often accompanied by flank pain
Acute Uric Acid Nephropathy tumor lysis syndrome deposition of uric acid crystals in the kidneys and their collecting systems, leading to partial or complete obstruction of collecting ducts, renal pelvis, or ureter. acute renal failure In the early phase uric acid crystals can be found in urine microscopic or gross hematuria Hyperuricemia urine uric acid/creatinine ratio >1 mg/mg (0.7 mol/mol)
Light Chain Cast Nephropathy • Patients with multiple myeloma may develop acute renal failure in the setting of : - hypovolemia, infection, or hypercalcemia or after exposure to NSAIDs or radiographic contrast media • The diagnosis of light chain cast nephropathy (LCCN)—commonly known as myeloma kidney—should be considered in : - patients who fail to recover when the precipitating factor is corrected - in any elderly patient with otherwise unexplained acute renal failure
Light Chain Cast Nephropathy • filtered monoclonal immunoglobulin light chains (Bence-Jones proteins) form : - intratubular aggregates - giant cell or foreign body reaction - direct toxicity to proximal tubular cells - intracellular crystal formation
Diagnosis • Clinical clues to the diagnosis include anemia, bone pain, hypercalcemia • Serum and urine should both be sent for protein electrophoresis
Chronic Tubulointerstitial Diseases interstitial fibrosis inflammatory cells are typically mononuclear abnormalities of the tubules tend to be more widespread, as evidenced by atrophy, luminal dilatation, and thickening of tubule basement membranes.
nonspecific nature The urine sediment is also unlikely to be diagnostic, except in allergic forms of acute tubulointerstitial disease in which eosinophils may predominate in the urinary sediment
Defects in renal function Proteinuria ( predominantly of low-molecular-weight proteins, is usually modest, rarely > 2 g/d ) Defects in urinary acidification and concentrating ability Hyperchloremic metabolic acidosis nocturia and polyuria. Proximal tubule dysfunction (fanconi syndrome) hypokalemia, aminoaciduria, glycosuria, phosphaturia, uricosuria, bicarbonaturia(RTA)
Chronic Tubulointerstitial Diseases Vesicoureteral reflux Sickle cell disease Chronic exposure to toxins Metabolic Disturbances Cystic and Hereditary Disorders Miscellaneous
Vesicoureteral Reflux and Reflux Nephropathy • urologic anomalies in early childhood • recurrent urinary tract infections • high-pressure sterile reflux may impair normal growth of the kidneys + recurrent UTIs • patchy interstitial scarring and tubular atrophy
Vesicoureteral Reflux function of the ureterovesical junction is impaired voiding cystourethrography may be required for definitive diagnosis Substantial proteinuria is often present
TOXINS Exogenous Toxins Analgesic Nephropathy Lead Nephropathy Metabolic Toxins Chronic Uric Acid Nephropathy Gouty Nephropathy Hypercalcemic Nephropathy
Analgesic Nephropathy renal function usually declines gradually papillary necrosis (hematuria -renal colic). sterile pyuria unable to generate maximally concentrated urine Distal RTA and nephrocalcinosis anemia the kidneys usually appear bilaterally shrunken on intravenous pyelography, and the calyces are deformed. "ring sign" on the pyelogram is pathognomonic of papillary necrosis CT may reveal papillary calcifications surrounding the central sinus complex in a "garland" pattern Transitional cell carcinoma may develop in the urinary pelvis or ureters as a late complication of analgesic abuse.
Lead Nephropathy occupational exposure accumulation of lead within renal cells proximal tubule dysfunction kidneys become atrophic Urinary excretion of lead may be increased hyperuricemi Acute gouty arthritis (so-called saturnine gout) develops in about 50% of patients with lead nephropathy Hypertension triad of "saturnine gout," hypertension, and renal insufficiency
Therefore, in any patient with: slowly progressive renal failure atrophic kidneys gout hypertension the diagnosis of lead intoxication should be considered measuring urinary lead after infusion of a chelating agent or by radiographic fluoroscopy of bone
Gouty Nephropathy Patients with less severe but prolonged forms of hyperuricemia presence of crystalline deposits of uric acid and monosodium urate salts in kidney parenchyma. proteinuria diminished urinary concentrating ability Early in its course, GFR may be near normal,
Hypercalcemic Nephropathy • Chronic hypercalcemia is seen in Hyperparathyroidism Sarcoidosis Multiple myeloma Vitamin D toxicity Metastasis bone disease
Hypercalcemia decrease GFR through renal vasoconstriction • Calcium deposition in distal nephron and interstitial that leads to mononeuclear cell infiltration and tubular necrosis • Defective concentration ability, poliuria, nocturia • Nephrocalcinosis & nephrolitiasis
Radiation Nephritis if 23 Gy (2300 rad) of x-ray irradiation is administered to both kidneys. acutely or chronically renal failure moderate to malignant hypertension anemia proteinuria that may reach the nephrotic range Malignant hypertension without renal failure may follow unilateral renal irradiation and resolve with ipsilateral nephrectomy
WBC Casts Cells in the cast have nuclei (unlike RBC casts) Pathognomonic for Acute Interstitial Nephritis
Question • 1. 65 year old with H/o HTN, ventricular arrythmias controlled on Amiodarone, OA on NSAIds presents with puffiness on face on waking up. Has bilateral pitting dema. UA 3+ prot, 3 RBC., 15-20 WBC • 24 h prot – 4 g/day • BUN/creat 80/5 • Serum albumin 2.8, TSH normal. The most likely diagnosis? • A) amiodarone induced hypothyroidism • B) RPGN • C) NSAIDs induced nephrotic sdr and interstitial nephritis
1. hyaline casts 2. muddy brown casts 3. RBCs 4. RBC casts 5. Oval fat bodies 6. eosinophils A. ATN B. prerenal azotemia C. glomerulonephritis D. nephrolithiasis E. interstitial disease F. nephrotic syndrome Match:
1. hyaline casts 2. muddy brown casts 3. RBCs 4. RBC casts 5. Oval fat bodies 6. eosinophils A. ATN B. prerenal azotemia C. glomerulonephritis D. nephrolithiasis E. interstitial disease F. nephrotic syndrome Match: