Download
1 / 25
1.16k likes | 4.06k Views
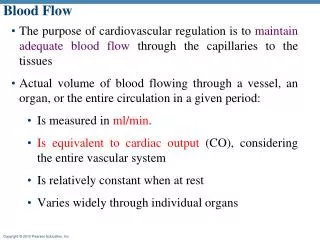
Cerebral Blood Flow. Richard Klabunde, Ph.D. September 11, 2003. Outline. Vascular anatomy of brain Control of cerebral blood flow Determinants of cerebral perfusion pressure Local regulation of cerebral blood flow Regulation of CBF by arterial pO 2 and pCO 2 Neurohumoral regulation

E N D
Cerebral Blood Flow Richard Klabunde, Ph.D. September 11, 2003
Outline • Vascular anatomy of brain • Control of cerebral blood flow • Determinants of cerebral perfusion pressure • Local regulation of cerebral blood flow • Regulation of CBF by arterial pO2 and pCO2 • Neurohumoral regulation • Cushing reflex • Control by neuropeptides • Conditions related to altered cerebral blood flow
Vascular Anatomy Circle of Willis (From E. Gardner, Fundamentals of Neurology. W.B. Saunders, 1963)
Cerebral Blood Flow(Basic Facts) • ~15% of cardiac output to only 2% of body weight • Blood flow supports an O2 consumption that is almost 20% of whole body O2 consumption at rest in adults (higher in infants) • Cerebral blood flow is relatively high on a tissue weight basis: 50-60 ml/min/100g (cp. 80 ml/min/100g in heart) • A-V O2 extraction is about 6 ml O2/100 ml blood • Because of the rigid cranium, blood volume is nearly constant – this has important implications when hemorrhagic strokes occur and when intracranial pressures rise
Cerebral Perfusion Pressure (normally 0-10 mmHg)
Coupling Between Cerebral Blood Flow and Brain Activity • The brain has an absolute requirement for O2 (for glucose oxidation) and has little anaerobic capacity • Reduction in blood flow (relative ischemia) impairs O2 delivery and causes cerebral hypoxia • Recall, O2 delivery = Flow x Arterial O2 Content • Recall, O2 consumption = Flow x (AO2-VO2 ) • Unconsciousness results after only a few seconds of oxygen deprivation • Therefore, blood flow and metabolism need to be tightly coupled
Functional Hyperemia • Total brain blood flow is tightly coupled to cerebral oxygen consumption • Changes in mental activity alter oxygen consumption, which then either increases or decreases blood flow • Changes in activity in specific brain regions leads to parallel changes in blood flow to those regions
Functional Hyperemia cont. Cerebral Blood Flow Coma Awake Seizure Increasing Oxygen Consumption
Mechanisms of Functional Hyperemia pO2 • VO2 pCO2 H+ K+ Arteriolar Vasodilation ? Adenosine NO
Cerebral Autoregulation (Description) Headaches BBB disruption Edema Cerebral Hypoxia Cerebral Blood Flow Autoregulatory Range 0 100 200 Mean Arterial Pressure (mmHg)
Cerebral Autoregulation (Autoregulatory Shift) Normal Cerebral Blood Flow Chronic Hypertension Acute Sympathetic Stimulation 0 100 200 Mean Arterial Pressure (mmHg)
Cerebral Autoregulation(Possible Mechanisms) • Metabolic • Decreased perfusion pressure leads to: • pO2 (decreased O2 delivery) • pCO2 (decreased CO2 washout) • H+ (decreased H+ washout plus lactic acid) • adenosine (hypoxia resulting in net loss of ATP) • ? • Each of the above changes produces vasodilation • Myogenic • Decreased perfusion pressure decreases stretching of arteriolar smooth muscle which causes relaxation
Effects of Arterial pO2 • Systemic arterial hypoxia (pO2 < 50 mmHg) causes cerebral vasodilation and increased flow • Similar to the coronary circulation, although coronaries are more sensitive to decreased pO2 • Unlike renal, splanchnic, and muscle circulations where systemic hypoxia causes sympathetic-mediated vasoconstriction
Effects of Arterial pO2 100 Cerebral Blood Flow (ml/min•100g) 50 0 0 100 200 Arterial pO2 (mmHg) (From Lassen, N.A., Brain. In: Peripheral Circulation, P.C. Johnson, ed. Wiley, 1978)
Effects of Arterial pCO2 • Increased arterial pCO2 (hypercapnea) causes cerebral dilation • CO2 diffuses through blood-brain barrier into the CSF to form H+ (via carbonic acid) which then causes the vasodilation • Decreased arterial pCO2 as occurs during hyperventilation causes cerebral vasoconstriction, decreased blood flow, and cerebral hypoxia
Effects of Arterial pCO2 100 Cerebral Blood Flow (ml/min•100g) 50 0 0 20 40 60 80 Arterial pCO2 (mmHg) (From Lassen, N.A., Brain. In: Peripheral Circulation, P.C. Johnson, ed. Wiley, 1978)
Autonomic Control • Sympathetic • Innervation from superior cervical ganglion primarily to larger cerebral arteries on brain surface • Very weak sympathetic vascular tone • Sympathetic blockade has little effect on flow • Maximal sympathetic stimulation increases resistance by 20-30% (cp >500% in muscle) • Shifts autoregulatory curve to right • Parasympathetic • Innervation from facial nerve (VII) • Weak dilator effect on pial vessels • Baroreceptor reflexes • Very weak
Sympathetic Control 100 Cerebral Blood Flow (ml/min•100g) 50 0 None Maximal Level of Sympathetic Activity (From Lassen, N.A., Brain. In: Peripheral Circulation, P.C. Johnson, ed. Wiley, 1978)
Effects of Intracranial Pressure(CNS Ischemic Reflex) • Increased intracranial pressure leads to mechanical compression of cerebral vasculature and decreased flow • Increased intracranial pressure elicits arterial hypertension (“Cushing reflex”) • May be caused by bulbar ischemia, which in turn stimulates medullary cardiovascular centers and increases sympathetic outflow to systemic vasculature • Bradycardia often accompanies the hypertension because of baroreceptor activation of vagal efferents to the heart
Humoral Control • Catecholamines • Weak alpha-adrenergic vasoconstriction is masked by autoregulation although very high doses of epinephrine can decrease flow • Beta-adrenoceptors cause vasodilation; however, this is masked by autoregulation • Angiotensin II • Very little or no effect
Neuropeptides and Other Vascular Control Mechanisms • Vasodilation • Calcitonin gene-related peptide (CGRP) • Substance-P • Vasoactive intestinal peptide (VIP) • Vasoconstriction • Neuropeptide-Y (NPY) • Endothelin (vascular and neuronal ET-1 and neuronal ET-3 acting primarily on ETA receptors)
Conditions Related to Altered Cerebral Circulation • Syncope • Hypotension • Orthostatic • Vaso-vagal reflex
Stroke • Hemorrhagic • Ruptured aneurism • Vascular weakening due to chronic hypertension • Ischemic • Thrombus formation or embolism • Vasospasm (ET-1?) associated with subarachnoid hemorrhage
Headache • Associated with (not caused by) neurovascular-mediated vasodilation in migraine and cluster headaches • Possible roles for CGRP and VIP