Download
1 / 10
110 likes | 239 Views
1 of 2. Impact of double dose vs standard dose oseltamivir on clinical and virological outcomes in pts with severe influenza. Multi-centre, double-blind RCT (South East Asia; 2007-2010)

E N D
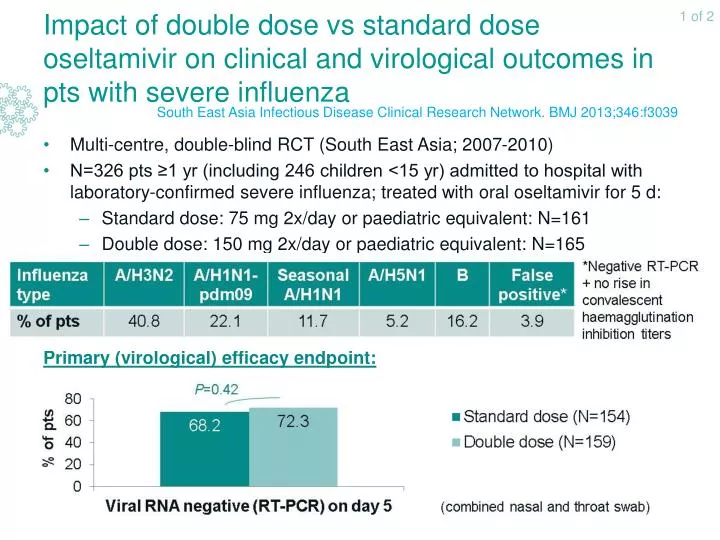
1 of 2 Impact of double dose vs standard dose oseltamivir on clinical and virological outcomes in pts with severe influenza Multi-centre, double-blind RCT (South East Asia; 2007-2010) N=326 pts ≥1 yr (including 246 children <15 yr) admitted to hospital with laboratory-confirmed severe influenza; treated with oral oseltamivir for 5 d: Standard dose: 75 mg 2x/day or paediatric equivalent: N=161 Double dose: 150 mg 2x/day or paediatric equivalent: N=165 Primary (virological) efficacy endpoint: South East Asia Infectious Disease Clinical Research Network. BMJ 2013;346:f3039
2 of 2 Impact of double dose vs standard dose oseltamivir on clinical and virological outcomes in pts with severe influenza Double dose oseltamivir does not seem to have virological or clinical advantages over standard dose in severe influenza pts South East Asia Infectious Disease Clinical Research Network. BMJ 2013;346:f3039
1 of 2 Spatial distribution of influenza virus aerosols generated by symptomatic patients Single-centre study (2010-2011 influenza season) N=94 pts (>2 yr) admitted to the emergency department (N=52) or inpatient care unit (N=42) and screened for influenza-like illness (i.e. documented fever (≥37.8°C) or patient-reported fever in past 12h, cough/sour throat and suspected influenza) Influenza virus in nasopharyngeal swab specimens detected by: Bedside rapid testing + Real-time RT-PCR Assessment of airborne dispersal pattern: 3x 6-stage Andersen air sampler placed facing the participant (lying in bed, but free to move the head) at head level at distances of ≤0.305 m (1 foot), 0.914 m (3 feet) and 1.829 m (6 feet); 20 min air sampling (no aerosol-generating procedures during sampling) Aerosolised influenza virus emitters: N=26 (43% of pts), including 5 pts with aerosolised influenza virus concentrations > high airborne human infectious dose (HID50: 1,950 RNA copies per 10 l human respiratory minute volume) Bischoff WE et al. J Infect Dis 2013;207:1037-46
2 of 2 Spatial distribution of influenza virus aerosols generated by symptomatic patients • Number of particles <4.7 µm diameter significantly decreased with increasing distance from patient’s head Infectious doses of influenza virus may be found up to 1.829 m from pts during non-aerosol-generating patient-care activities, predominantly in small particles (<4.7 µm diameter) Bischoff WE et al. J Infect Dis 2013;207:1037-46
1 of 2 Comparison of clinical characteristics between influenza A and B infections in hospitalised adults Retrospective study using Influenza Hospitalisation Surveillance Network (FluSurv-NET; USA): N=12,004 adults hospitalised for laboratory-confirmed influenza during influenza seasons 2005-2006 through 2011-2012 Influenza A: N=9,937 (83%) − influenza B: N=2,067 (17%) Comparison of clinical characteristics between pts with influenza A and B (April 2009-April 2010 pandemic period excluded, due to limited circulation of influenza B) Su S. IDWeek 2013 abs. 887 Data from poster
2 of 2 Comparison of clinical characteristics between influenza A and B infections in hospitalised adults No significant differences between both groups, except for antiviral treatment (Tx): A: 70% vs B: 57%; crude OR:1.8; 95% CI: 1.57-2.08 Comparison of clinical outcomes between virus types after oseltamivir Tx (2008-2009 influenza season excluded because of widespread oseltamivir resistance among seasonal influenza A virus) • Mortality after oseltamivir Tx: no sign. ≠ between virus types Influenza A and B infections resulted in similar hospital courses, although influenza A may cause more ICU admissions for adults <65 yr. Oseltamivir Tx outcomes were similar for both virus types Su S. IDWeek 2013 abs. 887 Data from poster
1 of 2 Effectiveness of 13-valent pneumococcal conjugate vaccine (PCV13) in reducing pneumococcus-related disease burden March 2010: 7-valent PCV (PCV7) replaced by PCV13 for paediatric use in USA → 2 years since implementation Methods: Private 20% inpatient ICD9-coded database projected to national figures: reviewing of electronic health records from hospital discharges Modelling of medical claims data to assess trends in uptake of PCV13 vaccine doses in children <5 yr For 2005-2012: modelling of monthly numbers of invasive pneumococcal disease (IPD), lobar pneumonia, empyema and all-cause pneumonia hospitalisations, controlling for influenza incidence Computing of PCV13-attributable risk reduction by age Mid-winter 2011-2012: About 50% of all children <5 yr: putatively protective PCV13 doses Simonsen L. IDWeek 2013 abs. LB3
2 of 2 Effectiveness of 13-valent pneumococcal conjugate vaccine (PCV13) in reducing pneumococcus-related disease burden 22,000 paediatric pneumonia hospitalisations avoided Introduction of PCV13 led to substantial reductions in invasive and non-invasive pneumococcus-related hospital admissions after only 2 yr Simonsen L. IDWeek 2013 abs. LB3
1 of 2 Efficacy of interferon-α2b (IFN-α2b) and ribavirin for Middle East respiratory syndrome coronavirus (MERS-CoV) in rhesus macaques Animal study: rhesus macaque = only known model organism for mild-to-moderate MERS-CoV infection, developing widespread pneumonia with transient clinical disease N=6 healthy rhesus macaques inoculated with 7x106 TCID50 MERS-CoV (combined intratracheal, intranasal, oral and ocular routes) Treatment: from 8h until 72 h after infection: N=3: Ribavirin + interferon (IFN)-α2b: Ribavirin: 30 mg/kg iv loading dose; then 10 mg/kg every 8h im Human IFN-α2b: 5 MIU/kg every 16h sc N=3: Sham: comparable volume/kg of sterile saline Animals monitored 3x/day: clinical scoring and/or examinations Day 3 after infection: necropsy Falzarano D et al. Nat Med 2013;doi:10.1038/nm.3362
2 of 2 Efficacy of interferon-α2b (IFN-α2b) and ribavirin for Middle East respiratory syndrome coronavirus (MERS-CoV) in rhesus macaques In MERS-CoV-infected rhesus macaques, treatment with IFN-α2b and ribavirin reduced virus replication, moderated the host reponse and improved clinical outcomes Falzarano D et al. Nat Med 2013;doi:10.1038/nm.3362