Download
1 / 30
430 likes | 943 Views
Radiation Protection. Review of Units of Measurements Protection for Patient and Personnel Review of Radiobiology Follows the ARRT Content Specifications. Sources of Radiation Exposure. Natural or background - ground, cosmic, naturally occurring isotopes, etc.

E N D
Radiation Protection Review of Units of Measurements Protection for Patient and Personnel Review of Radiobiology Follows the ARRT Content Specifications
Sources of Radiation Exposure Natural or background - ground, cosmic, naturally occurring isotopes, etc. Artificial or man-made - Medical and dental largest contributor to population dose
Units of Measurement - Know traditional andStandard International Units • Roentgen (R) - traditional unit of exposure in air - equipment related [x and gamma rays] Coulomb/Kg or C/Kg • rad (r) - traditional unit of absorbed dose [all] • Gray (Gy) • rem - traditional unit of dose equivalent [x, beta, gamma] • Seivert (Sv) • Curie (Ci) - measure ofradioactivity • Becquerel (Bq) = in Nuc Med
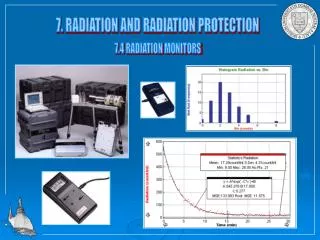
Film Badges - month photographic film TLD - 3 months Sensitive to 5 mrem Expensive Ionization chamber pocket dosimeter drifts / not accurate Larger one for NM or more industrial Ionization Counter Cutie Pie,Geiger Counter spills, more industrial Scintillation detector more technical use used in CT,NM Detection MethodsPersonnel Field Instruments
OSL • Aluminum Oxide • Laser beam releases light • Sensitive to exposures as low as 1 mrem • 3 months at a time • Can be reanalized
Monitoring Agencies • NCRP -National Council on Rad Protection • dose limitations control • DRH - Devices for Radiological Health • radiation control (more equipment related) • NRC - Nuclear Regulatory Commission - radiation protection standards (formerly- Atomic Energy Comm) • Maryland State Dept. Health & Hygiene • EPA - Environmental Protection Agency • more industrial application related matters
Recommendations for Dose • ALARA - As Low As Reasonably Achievable for patient and occupational worker • Cumulative Dose Limit for Occupational Worker - simply your age x 1 rem • ie. 47yo male RT, 47 rem • Embyro or fetus -- 50mrem/month or 500 mrem total • Member of public frequently, exposed 100mrem
Interactions with Matter • Coherent ( Classicial or Thompson) scattering: < 30kVp • Photoelectric Effect 30-150 kVp • Compton’s Scatter: 30-150 kVp • ie. 70kVp 40% PE and 60% Compton • vs 100kVp 10% PE and 90 % Compton • Pair Production and Photodisintegration : MeV as in Rad Therapy
Estimated Patient Doses • Skin - TLD 15, 000mrem and extremities 30,000 mrem • Gonad -- genetic responses at 20rads/yr • Bone Marrow (mean) - rad induced leukemia 100 rad/yr • Gonadal and bone doses are estimates!
Estimated Doses • Fluoroscopic are harder to measure • 2rad/mA/minute • remember patient becomes the hazard since the scatter is what gets the radiographer • Exams with higher patient doses are: • Fluoro • Angio • Portables • General - around pelvic region, hip femur, lumbar, coccyx, sacrum
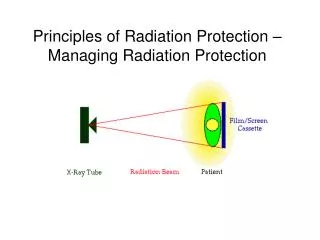
Cardinal Principles • Time : time, dose OR time, dose • Distance: distance, dose OR if you conversely distance, dose (don’t forget the inverse square law or direct square law) • Shielding: reduces dose as much as 95% in male patients
Cardinal Principles time, distance, shielding Exposure Factors kVp, mA, time, distance directly related kVp - interactions time - dose fluoro time -keep it short mA and (fast) time Filtration - inherent 0.5mm al <50kVp 1.5mm al 50-70kVp 2.5mm al >70kVp Film Screen Combo Beam limitation PBL - automatic collimation Cones Cylinders aperture diaphragms field, scatter, dose Avoid Repeats techniques charts good communication restraining devices good QA program Patient Protection
Shielding - not < 0.25mm Pb long bones in peds all eyes gonadal - 5cm primary flat rubber lead strips shadow shield shaped or cup eye shields If patient holds cassette, Pb glove needs to be 0.5 mm to protect hand Air Gap technique High Dose toGonads hip upper femur pelvis lumbar lumbo-scaral abdomen sacrum coccyx S-I Joints BE, IVP, Cysto, Hystero Patient Protection - continued
Cardinal Principles Time, Distance, Shielding Protective wear Pb aprons 0.5mm = Pb gloves 0.25mm = thyroid - dose 10% & 6mrad per exam Pb glasses 0.75mm dose 98% Pb sterile gloves Barriers - 7” high primary 1/16th inch secondary 1/32 inch Pb glass port mobile in OR Mobile exposure cord length - no less 6’ Personnel Protection
Never hold Patients - use immobilization devices Wear monitoring devices film badge TLD Pocket dosimeter Fluoro equipment - apron on tower, bucky slot cover, fluoro timer Clear room when doing portables or provide with Pb apron Stand 2 m from table Personnel Protection Continued
Radiographer self disclosure voluntary fetus 50mrem per month or 500 mrem or 5mSv over term Baby badge at waist 0.5mm Pb aprons are 88% effective > 70 kVp Patient ask about LMP ALARA double shield or limit exam views 10 day rule for high dose exams Pregnancy
Rad Protection - EquipmentGeneral Radiographic • Control panel: light, meters and sound • SID: within 2% variance • PBL: within 2% of SID • Beam alignment • Filtration: 2.5mm Al equivalent total • Reproducibility: output = , not to exceed 5% • Linearity: intensity = across mA stations, not be exceed 10% • Personnel shield: short cords so exposures are made behind 7” barriers
Rad Protection- EquipmentFluoro and Mobile • Mobile C-Arm: not < 12” (30cm) source to tabletop distance • Stationary Fluoro:not < 15” (38cm) source to tabletop distance • Primary Barrier: IA assembly 2mm Pb equivalent when >125kVp (usually 80-120 kVp fluoro) • Filtration: 2.5mmAl total just in overhead tube; <100mR/Hr leakage at 1 meter • PBL on Fluoro tower: borders on monitor when IA is 14” from tabletop • Exposure switch: “Dead man” - intermittent dose
Rad Protection - EquipmentFluoro and Mobile • Bucky Slot Cover: 5cm wide at gonadal level and 0.25mm Pb thick • Protective Apron on Tower: 0.15- 0.25mm Pb between patient & operator • Cumulative Timer for Fluoro: 5 min/audible • X-Ray Intensity: should not >2.1R/min at tabletop per mA at 80 kVp • Dose Rate: must not > 10R/min maximum, should not 5 • Front loaded cassette vs back load: front less dose • Spot cassette vs spot film camera -- dose to patient 3x more for cassette over camera
RADIOBIOLOGY In addition to the technical side, we must understand the biological effects!
Characteristics of Radiation • Physical • LET - efficiency of radiation to produce excitation and ionization ( energy deposit per unit path length) • LET of dx is 3 keV/m • RBE - Relative Biological Effectiveness
Biological Aspects • Review the mitosis and meiosis cycles • The most sensitive time for DNS is G2 and rest of mitotic stages (least during G1 and Synthesis) • Keep in mind that in meiosis, DNS replicates only once • What about other factor affecting cellular response?
Laws of Sensitivity • High mitotic activity -- more sensitive • Cell differentiation -- less, more sensitive • Long dividing future -- more sensitive • All these Bergonie and Tribondeau • Biological Stress • Pre/post irradiation conditions • Chemicals -- enhancers, protectors • Ancel and Vitemberger -- more environment related
Effects--- • Direct - photon strikes DNA --breaks in ladder either rungs or side rails • Indirect - photon strikes water -- most abundant so most likely to happen more frequently • Target Theory -- variations, but striking a critical DNA area where lethality occurs immediately or may take two hits to achieve death • Cell survival curves - curve representing the dose and proportion of cells surviving
Mean Survival Curves • Relationship between the dose and number of cells that survive • Lethal Dose • human LD 50/60 -- 350 rad • previously 50/30 - Chernobyl changed figures
Dose Response Relationships • Linear, non-linear • Threshold or non-threshold • (non-stochastic) (stochastic, random) • We practice by Linear, non-threshold
Cellular Responses • Interphase death • Division Delay • Reproductive failure
Stages of ResponseDose Dependent • Prodromal -- NVD • Latent • Manifest • hematologic --dose between 100-1000 • 200-600/200-1000 • GI syndrome - dose between 1000-5000 • 600-1000 • CNS - dose > 5000 • Recovery or Death
Radiation Reduced Malignancy • Historical populations • Dose related • Risks associated • 20% population USA will die of Ca • how do you tell if rad caused? • Children? Leukemia is common
In Utero -- Fetal Irradiation • neonatal death - 2-3 week of gestation • malformations • growth stunting • congenital defects - functional defects after week 20 • cancer induction • Week 4-11 severe abnormalities, especially CNS and skeletal, while 11- 16 mental retardation & microcephaly