Download
1 / 52
540 likes | 563 Views
Liver Functions and Disorders. One of the most important organ Largest organ that can regenerate itself. Blood supply (Dual Blood Supply). Hepatic artery (25% of liver’s blood flow) – Oxygenated Portal vein (75%). Anatomic Structure of the Liver.

E N D
Liver Functions and Disorders • One of the most important organ • Largest organ that can regenerate itself. • Blood supply (Dual Blood Supply). • Hepatic artery (25% of liver’s blood flow) – Oxygenated • Portal vein (75%).
Anatomic Structure of the Liver • Liver is divided into 2 lobules, which contain hepatocytes. • Portal vein drains through the GI system. • Hence any problem with GI system will affect the liver • Interference with these blood supplies by fibrosis as in cirrhosis will cause portal hypertension.
Hepatocytes are the cells of the liver and very important for hepatic functions. • Bile drains through the bile duct and any blockage will cause obstructive jaundice • Sinusoidal lining cells include endothelial cells involved in endocytosis • Cupffer cells are mainly involved in phagocytosis and immune response (RE function) • Ito cells-(perisinusoidal fat storing cell) store matrix proteins and are involved in fibrosis. • Extracellular matrix include collagen involved in fibrosis
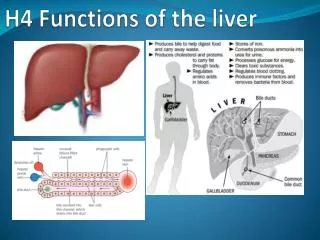
FUNCTIONS OF THE LIVER • Synthetic function ( e.g. Some plasma proteins, 10 bile acids) • Excretory function (Bilirubin) • Detoxification function ( Xenobiotics) • Metabolic function ( Metabolism of macronutrients/macromolecles)
Metabolic/Synthetic functions of the Liver • The liver plays a major role in the matabolism of macronutrients (e.g.carbohydrate, lipid and protein. • Glycolysis, the Krebs cycle, gluconeogenesis, glycogenesisand glycogenolysis, lipogenesis, ketogenesis, amino acid synthesis and degradation, and protein synthesis all take place in the liver. • Hepatocytesalso metabolise and detoxify endogenous (haem) and exogenous products (drugs), which are then excreted via the biliary tree.
Secretory/Excretory Function of the Liver BILIRUBIN METABOLISM : Sources of bilirubin include: • RBC breakdown: 90% of RBC breakdown occurs within RES cells (mainly in spleen) • Ineffective erythropoiesis (in bone marrow) • Other haem containing proteins e.g. myoglobin and cytochrome P450 (mainly in liver).
70 to 80% of daily bilirubin production is derived from the breakdown of senescent red blood cells • The remainder is derived from ineffective erythropoiesis and the breakdown of other haem-containing proteins. • Total daily bilirubin production is 450 to 550 μmol/day.
FORMATION OF BILIRUBIN • Haemoglobin is broken down to globin and haem. • Globin (a protein) is broken down to its constituent amino acids. • Haem (a 4 ring structure containing Fe at its centre) is broken down (via biliverdin) to carbon monoxide, iron and bilirubin. • Biliverdin gives the green colour sometimes seen in a resolving bruise. • The bilirubin at this stage is termed unconjugated bilirubin because it has not yet been processed by conjugation in the liver.
Unconjugated bilirubin is: • A hydrophobic molecule. • Strongly bound to hydrophobic sites on albumin. • Can be displaced from binding sites on albumin by drugs (salicylates, sulphonamides). • Does not appear in urine. • Free unconjugated bilirubin is normally <3 μmol/l. • Free unconjugated bilirubin is neurotoxic. • Is deposited in cell membranes (esp. basal ganglia) at high concentration and causes kernicterus.
Uptake of Unconjugated Bilirubin by the Liver: • The unconjugated bilirubin - albumin complex is carried in the plasma to the hepatic sinusoids, enters the space of Disse and dissociates at the hepatocyte membrane. • It is taken up by the hepatocytes by a carrier-mediated process. • Within the hepatocyte the unconjugated bilirubin is bound to ligandin.
Conjugation of Bilirubin by the Liver • The bilirubin is then conjugated with glucuronic acid by UDP-glucuronyltransferase (UDPGT I) to bilirubin monoglucuronide (BMG) and by UDPGT II to bilirubin diglucuronide (BDG). • Conjugated bilirubin is more water soluble and can be excreted in bile or urine. • Under normal circumstances there is no conjugated bilirubin present in plasma
Excretion of Bilirubin into Bile • Conjugated bilirubin is transported out of the liver cells into the bile canaliculi by an energy-dependant carrier-mediated process which is sensitive to cell injury. This canalicular excretion step rather than conjugation is thought to be the rate-limiting step in bilirubin metabolism. • Bile flows through the canaliculi, into the bile ducts, and finally into the duodenum.
UROBILINOGEN • In the GIT, bacterial flora convert conjugated bilirubin to urobilinogen. • Most of the urobilinogen (colourless) is further converted by colon bacteria to urobilin and stercobilin (brown). • In the absence of bowel flora (newborns, broad spectrum antibiotic therapy) faeces are yellow due to bilirubin. • 20% of urobilinogen in the small intestine is reabsorbed into the portal circulation, taken up by the liver again and re-excreted (enterohepatic circulation). • Some urobilinogen appears in normal urine. Easy to test with dipstick. • Re-uptake of urobilinogen by the liver is sensitive to liver damage.
Increased urine urobilinogen can be due to: 1. Increased bilirubin production (haemolysis) 2. Liver disease (but not if obstruction prevents bilirubin reaching GIT).
Bile Acid (= Bile Salt) Metabolism • The products of cholesterol metabolism are chenodeoxycholic acid and cholic acid, known as primary bile acids (From Liver). • The rate limiting and regulated step in their formation is 7-α-hydroxylation of cholesterol. • Prior to secretion into the bile canaliculi, the primary bile acids are conjugated to glycine or taurine . • Conjugated bile acids are transported out of the liver cells into the bile canaliculi by an energy-dependant carrier-mediated process
In the GIT, bacterial enzymes deconjugate and α-dehydroxylate the primary bile acids and convert them to the 2O bile acids- lithocholic acid and deoxycholic acid. • Most of the bile acids in the GIT are reabsorbed into the portal circulation ,taken up by the liver again and re-excreted (enterohepatic circulation). • Re-uptake of bile acids by the liver is highly efficient, but sensitive to liver damage.
Circulation of Bile Acids • Bile acids in the GIT are reabsorbed into the portal circulation and transported back to the liver, but a small fraction may escapes re-absorption by the liver and appears in the systemic circulation. • i) If there is obstruction in the biliary tree, back-pressure causes reflux of bile acids from the liver directly back into the systemic circulation, causing constant high systemic bile acid concentrations, with the side effect of severe pruritus (itching).
ii) If there is liver damage with impaired re-absorption of bile acids from the portal circulation, more bile acids than normal appear in the systemic circulation after a meal, and are gradually re-absorbed. • iii) If there is ileal disease, bile acids are excreted and not re-absorbed, resulting in constant low systemic levels.
STRUCTURE OF BILE ACIDS • Bile acids are amphipathic molecules, with all the hydroxyl groups oriented on the same side of the plane. • Thus one side is hydrophilic (due to -OH groups), the other hydrophobic (due to steroid nucleus), which gives detergent properties. • This facilitates the formation of micelles when mixed with triglyceride or other lipids, and allows lipid absorption.
FUNCTIONS OF BILE ACIDS: 1. Solubilise cholesterol for excretion. 2. Solubilise dietary fat for absorption. 3. Stimulate bile formation and flow.
Pathophysiology of liver Disease 1. Exposure to toxic agents such as drugs Two forms of reactions are possible: • Predictable reaction, which is dose-depednent (e.g. Hepatoxicity) as seen in CCl4 poisoning. • Unpredictable reaction, which include idiosyncratic and not dose-dependent. Other toxic agents include viruses bacteria fungi and protozoa
2. Obstruction of bile flow: this could be from biliarystenosisor any cause of obstruction, which could be extrahepatic or intrahepatic 3. Vascular Disturbances: Hepatic artery could be occluded leading to infarction. Could be pre-, intra- or post hepatic obstruction. 4. Disturbed immunity: Chronic active hepatitis due to HBV will lead to non-recognition of hepatocytes and their subsequent destruction.
5. Primary pancreatic disease: Cystic fibrosis (exocrine pancreatic disorder, which also affects the respiratory system and GIT. 6. Developmental abnormality: many congenital problems such as polycystic disease ( cyst in the liver, kidneys and brain) 7. Abnormal storage of substances in the liver: Extra-& Intracellular deposition of amyloid, fats, glycogen etc.
8. Disturbed metabolic function: Could be due to enzyme defects e.g., galactoasemia, glycogen storage disease. 9. Tumours: Could be benign (hepatic cell adenoma) or malignant (hepatocellular cancer) 10. Granulomatous hepatitis: This could be due to viruses, TB etc.
11. Post-operative liver disorders: many forms due to anaestesia, ischaemia or mixed hyperbilirubinaemia 12. Idiopathic: Of unknown origin
Biochemical Tests of Liver Cell Integrity and Function BILIRUBIN Bilirubin is usually measured by the JendrassikGrof modification of the van den Bergh reaction: • conjugated bilirubin (direct-reacting) • unconjugated bilirubin (indirect-reacting). • Normal serum total bilirubin <17 μmol/l (all unconjugated). • Normal urine contains no bilirubin. • Bilirubin only appears in urine when conjugated bilirubin is elevated in plasma.
Increased amounts of unconjugated bilirubin are found in plasma in: • Increased bilirubin production • Decreased uptake or conjugation of bilirubin • In generalised hepatocellular dysfunction • In specific rare inherited syndromes (Gilbert’s and Criggler-Najjar syndromes).
Increased amounts of conjugated bilirubin are found in the plasma (and urine) in: • Decreased excretion of bilirubin • In obstructive liver disease • In specific rare inherited syndromes (Rotor’s and Dubin-Johnson syndromes).
URINE UROBILINOGEN • Urine urobilinogen is measured qualitatively using a dipstick. • Normal urine contains some urobilinogen. Increased amounts of urobilinogen are found in the urine in: • Increased bilirubin production. • Decreased re-uptake into liver due to hepatocellular dysfunction (but not if obstruction prevents bilirubin reaching GIT).
LIVER ENZYMES • The usefulness of serum enzymes as markers of liver disease is limited by the fact that they are also found in and released from other tissues. • It is therefore more useful to look at all the parameters of liver function (or at least all of the enzymes) rather than one single enzyme.
Enzymes Reflecting Liver Cell Damage These enzymes are released from damaged cells, due to increased cell membrane permeability or cell necrosis. These include: 1. Transaminases: • AST; No tissue-specific isoenzymes. Cytosolic and mitochondrial. • ALT is more liver-specific. Cytosolic only. • LD or LDH has widespread tissue distribution including liver, red blood cells, skeletal and cardiac muscle. • Tissue-specific isoenzymes; LD5is found in liver and skeletal muscle only.
Enzymes Reflecting Cholestasis: • ALP; has widespread tissue distribution including liver, bone, placenta and GIT. The liver isoenzyme can be identified by electrophoresis or heat inactivation. It is released into plasma in cholestasis. • Gamma-glutamyltranspeptidase (GGT) is more liver-specific. • Involved in the transport of amino acids across the liver cell plasma membrane. • Serum level increased by cholestasis or chronic ingestion of alcohol, barbiturates, phenytoin and other drugs which induce the enzyme.
\Plasma Proteins • Albumin is decreased in chronic liver disease, but is insensitive as an index of liver function (long half-life of18 days). • Clotting factors have short half-lives; Prothrombin time and partial thromboplastin time (PTT) may be prolonged in liver disease. • Immunoglobulins show a generalised increase (polyclonal) in chronic liver disease, especially cirrhosis. • In primary biliary cirrhosis IgM is characteristically increased. • In alcoholic cirrhosis IgA is characteristically increased and this tends to cause "beta-gamma bridging" on serum electrophoresis.
In autoimmune chronic active hepatitis IgG is particularly increased. • AFP is the embryonic form of albumin, normally absent from plasma but increased markedly in primary liver cell carcinoma (hepatoma). • Also produced by some germ cell tumours (e.g. teratoma). • Moderate elevations may occur when liver tissue is regenerating, such as in the recovery stage after hepatitis or in cirrhosis.
Liver Disorders and Jaundice • Jaundice or icterus is the yellow appearance of skin and sclerae due to the presence of an excessive amount of bilirubin. • Jaundice becomes clinically visible when serum bilirubin is >40 μmol/l). • The liver has a large reserve capacity - jaundice only appears with severe impairment of liver function.
JAUNDICE • Yellowish discolouration of mucus membrane and the conjunctiva when plasma bilirubin exceeds 50µmol/L • Jaundice (Hyperbilirubinaemia) may be • Prehepatic • Hepatic or • Post hepatic
PREHEPATIC JAUNDICE • Usually due to overproduction of bilirubin • Leads to increased unconjugated bilirubin • Common causes are: • Haemolytic anaemia • Haemolytic dx of the new born • Ineffective erythropoiesis e.g. hereditary spherocytosis • Bleeding into tissue- rhabdomyolysis ( Sports injury)
HEPATOCELLULAR JAUNDICE* • Usually from drugs and toxins • And as a late complication of cirrhosis • Gilbert’s dx- low activity of UDP glucuronyl transferase • a familial autosomal dominant, commoner in men • Leads to failure of uptake and conjugation of bilirubin • Presents as assymptomatic unconjugated hyperbilirubinaemia
CRIGLER NAJAR SYNDROME • A rare condition leading to severe unconjugated bilirubin • Due to low activity of UDP glucuronyltransferase • Presents as severe hyperbilirubinaemia in neonates leading to kernicterus
Dubin Johnson and Rotor* syndrome • Both are causes of conjugated hyperbilirubinaemia with bilibinuria • Results in defective transfer of conjugated bilirubin into the biliary canaliculi • Features include bilirubinuria • Plasma alkaline phosphatase is normal • The difference between the 2 conditions is the presence of pigmentation of hepatocytes and increased urinary coporphyrins in Rotors syndrome
CHOLESTASIS * • Could be intra hepatic or post hepatic • In both conditions , there is conjugated hyperbilirubinaemia and bilirubinuria • Cholestasis is encountered in acute hepatocellular damage, Cirrhosis, • Intrahepatic ca (secondaries to the liver) drugs such as phenothiazines, methyl testosterone • Extra hepatic causes are usually due to gall stones, ca head of pancreas, ca of biliary tree, biliary atresia
MARKERS OF CHOLESTASIS • ALP, GGT rise several times the normal level after several days of bile duct obstruction or intrahepaticcholestasis • In metastasis to the liver ALP is elevated >1000 I.U or > 6x URL • GGT is elevated in alcoholics >45g ethanol/day • ALP is also raised in growing children and bone inflammation. • ALP is also produced in the intestine and placenta
SYNTHETIC FUNCTION • Serum Albumin level is a marker of synthetic function and it is a valuable guide to the severity of chronic liver disease • A falling serum albumin in liver disease is a bad prognostic sign • In acute liver disease albumin levels may be normal
Prothrombin time (P.T.) B/c of its short half life (Approx 6 hrs), it is a sensitive indicator of both acute and chronic liver disease • When PT is prolonged vitamin k deficiency has to be excluded by intravenous bolus (10g) of vitamin k • Vitamin k deficiency commonly occurs in biliary obstruction as the low intestinal concentration of bile salts results in poor absorption of vitamin k.
MARKERS OF HEPATOCELLULAR DAMAGE • Soluble cytoplasmic enzymes and to a lesser extent mitochondria enzymes are released into the plasma in hepatocellular damage • The measurement of the of alanineaminotransferase (ALT )or aspartate amino transferase (AST) in plasma provide a sensitive index of hepatocellular damage from inflammation • Plasma ALT is more liver specific than AST
AST has both cytoplasmic and mitochondrial iso- enzymes and tends to be released more than ALT. • AST is also present in the heart, brain muscle, kidney, red cells therefore not specific • High level are obtained in hepatic necrosis myocardial infarction, muscle injury and congestive cardiac failure • ALT is a cytoplasm enzyme and is more specific to the liver although it is also present in the skeletal muscles.
MARKERS OF INFLAMMATION • ALT &AST values are higher in obese patients (Fatty liver) • ALT level declines with weight loss • Both enzymes are not sensitive markers of chronic liver disease