Download
1 / 20
200 likes | 207 Views
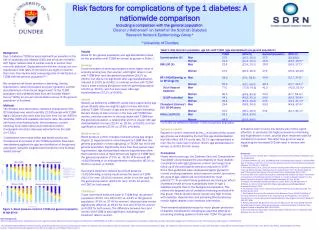
This article explores the risks and considerations for individuals with diabetes in workplace and recreational settings. It covers topics such as diabetes types, related issues, complications, and the impact on occupations and hobbies. It also emphasizes the importance of effective risk management, communication, and education to ensure safety.

E N D
Diabetes, risk and driving! Lorna Bingham NP
Overview • Risk & workplace risk • Diabetes T1 vs T2 • Diabetes related issues • Depression • Acute, Chronic complications • Occupations • Driving, cranes, fork lifts ,operating machinery, ladders etc • Hobbies • Kite boarding, diving, caving • Human factors
Considerations of work place risk Health & Safety at work ACT 2015 Control Measures Occupational Health risk reduction Hazards Identified Good Practice Plan & Education Managed Teamwork Evidence based Practice Assessment
Risk Management Principles and guidelines AS/NZS ISO 31000:2009 Risk- Context Accountability Communication Define risk criteria Risk assessment • Identify • Analysis • Evaluate • Treat
Worksafe - manage risk Provides an extensive range of industry-specific guidance about how to manage workplace risks for: • manufacturing • agriculture • forestry (there is a separate Safe Tree industry website) • construction and building • adventure activities • the extractives, geothermal, petroleum and energy sectors • asbestos • mining • major hazard facilities • work-related health (eg noise, silica, solvents).
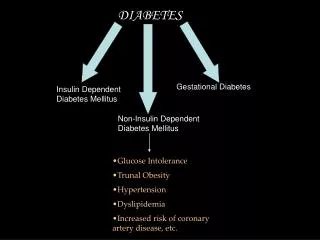
Diabetes comparison Type 1 – make no insulin Type 2 – make insulin but not working effectively Acute onset • 3 P’s- Polyuria, polydipsia, polyphagia, infections, blurred vision • Any age • Ketones Treatment • Need insulin injections from diagnosis Gestational Diabetes Mellitus (GDM) Other Insidious onset • Family Hx of T2DM or CVD • Obese BMI > 30 • Antipsychotic medications • Ethnicity Treatment • LIFESTYLE • Monitoring and follow up • Metformin, glipizide, gliclazide Anti HTNs , statins • Many will need insulin eventually
ContextOccupation & hobbies=concern Heights Water Other Working alone Equipment & machinery Chemicals Electricity
A comprehensive assessment framework reduces risk in diabetes • Family history • Psychosocial inc occupation & hobbies • Medication • CVD & HbA1c • Diagnosis Good communication lowers risk • Role and responsibility, • Health literacy
Diabetes risk – how do we manage it? • Diagnosis /misdiagnosis • Medication – insulin top 6 medications for errors • Acute complications & Management • Hypoglycaemia • Hyperglycaemia, HHS or DKA • Chronic complications result in hospitalization
Psychosocial Aspects of Diabetes • Clinical significant psychopathology is more common in those with diabetes • Depression – screen annually, women higher rate than men • Anxiety lifetime prevalence of 19.5% in T1 & T2 • Disordered Eating – screen if unexplained hyperglycaemia and weight loss • T1 insulin omission • T2 binge eating • Diabetes Distress & Fear of Hypos in T1
Diabetes Distress “Refers to significant negative psychological reactions related to emotional burdens and worries specific to an individuals experience in having to manage a severe, complicated and demanding chronic disease such as diabetes” Prevalence 18-45% Constant behavioural demands of medication dosing, testing, food intake (S45)
Driving Medical aspects of fitness to drive 2014 classes P135-137
Diabetes & Driving concerns • Hypoglycaemia - sudden onset • Test if not eaten, date and time correct on the meter & have Rx at hand • Hypoglycaemia unawareness – sudden cognitive impairment • ? Should they be driving – run bgls higher 6-12 • MUST test before drive and have Rx at hand • Hyperglycaemia - ?safe to drive • Blurred vision, neuropathy, CVD health, retinopathy
Diabetes Prevention • There is strong and consistent evidence that modest persistent weight loss can delay the progression from prediabetes to T2 Diabetes • See Diabetes Prevention Program 43% reduction in diabetes at 20 years • Benefit of weight loss of >5%, > 7% is optimal in lipids, BP and glycaemic control • 150 mins of moderate – vigorous exercise per week over 3 days and no more than 2 days with out activity
To Err is Human Report Institute of Medicine 1999 • 1:10 suffer unintentional harm in coming into hospitals • Due to “Human factors” • Be vigilant • Tell people with diabetes they are the experts and to question decisions if they do not seem right • Insulin is top 6 medications for errors • Knowledge is vital for reducing risk for people with diabetes (& health professionals!) • National Diabetes Nursing Knowledge & Skills Framework 2018
References • American Diabetes Association Standards of Medical Care in Diabetes 2018 • National Diabetes Nursing Knowledge & Skills Framework 2018 • https://www.diabetes.org.nz/managing-diabetes-driving/ • https://www.nzta.govt.nz/assets/resources/factsheets/16/docs/16-diabetes.pdf