Download
1 / 22
220 likes | 694 Views
LIVER. OVERVIEW. Tests for detecting: 1. Hepatocellular injury 2. Hepatic dysfunction 3. Cholestasis. 1.TESTS FOR DETECTING HEPATOCELLULAR INJURY. HEPATOCELLULAR INJURY.

E N D
OVERVIEW Tests for detecting: 1. Hepatocellular injury 2. Hepatic dysfunction 3. Cholestasis
HEPATOCELLULAR INJURY - It is detected by performing blood tests which measure the activity of the enzymes released “leak” from injured hepatocytes. - These tests: • Can assess the severity of the injury • Cannot differentiate reversible from irreversible, or local from diffuse injury.
TESTS FOR DETECTING HEPATOCELLULAR INJURY • Alanine aminotransferase (ALT) • Aspartate aminotransferase (AST) • Glutamate dehydrogenase (GLDH) • Sorbitol dehydrogenase (SDH)
Cytoplasm: ALT SDH AST(cytosolic isoenzyme) nucleus AST GLDH mitochondria LOCATION OF ENZYMES USED FOR DETECTING HEPATOCELLULAR INJURY hepatocellular membrane
ALT - ALANINE AMINOTRANSFERASE - High sensitivity - High liver specificity in dog & cat - Not useful for horse, ruminant, pig • (activity is too low to be measured accurately)
AST – ASPARTATE AMINOTRANSFERASE - Mainly used for diagnosis of liver disease in large animals - Relatively high sensitivity - Low liver specificity as also present in muscle and RBCs - May indicate more serious hepatocellular injury than ALT N.B. May indicate more serious injury than ALT, since part is located in mitochondria and will be released if the injury affects not only hepatocellular but also mitochondrial membranes.
CAUSES OF INCREASED SERUM AST ACTIVITY - Hepatocellular Injury - Muscle damage Interpret in conjunction with the muscle enzyme creatine kinase - Haemolysis (pathological or artefactual)
CAUSES OF INCREASED SERUM AST ACTIVITY • Muscle damage (AST can be markedly increased) • Hepatocellular damage: AST & Normal CK (in small animals ALT) • Muscle damage: AST & CK • Haemolysis (mild increase) • Red blood cells contain more AST than ALT • AST values higher than those of ALT in haemolysed samples
GLDH - GLUTAMATE DEHYDROGENASE - Moderate sensitivity - High liver specificity for all species - The increased serum GLDH activity is short lived Causes of increased serum GLDH activity: - Hepatocellular injury
SDH - SORBITOL DEHYDROGENASE - Liver specific - Must be tested within 8-12 hours of sampling - Increased serum SDH activity is short-lived Causes of increased serum SDH activity: - Hepatocellular injury
2. TESTS FOR DETECTING HEPATIC DYSFUNCTION • Hepatic Dysfunction is a pathological state due to marked reduction of functioning hepatocytes. • Can occur in hepatocellular disease, hypoplasia/atrophy of the liver or cholestasis.
TESTS FOR DETECTING HEPATIC DYSFUNCTION • Bilirubin (also a test of cholestasis) • Bile acids • Ammonia • Dye clearance tests • Liver enzymes can be normal despite severe liver dysfunction.
- Tests the ability of the liver to reabsorb bile acids from the portal vein Bile acids are: Synthesized in liver from cholesterol Conjugated mainly with taurine Excreted as sodium salts (bile salts) into gastrointestinal tract and used to digest fat Removed from the portal circulation by the liver. BILE ACIDS
FASTING BILE ACIDS - Serum sample obtained after 12h fast in small animals. - Increased due to: Cholestasis Spontaneous Gall Bladder contraction Hepatic dysfunction Portosystemic Shunts (PSS) - Fasting bile acids can be normal in cases of PSS or hepatic dysfunction
POST-PRANDIAL BILE ACIDS (PPBA) -Serum sample obtained 2h after feeding. This test is only valid in monogastric animals. -Increased due to: Hepatic dysfunction Portosystemic Shunts (PSS) Cholestasis -PPBA can increase: sensitivity (more PSS/hepatic dysfunction cases are detected) specificity (rules out spontaneous GB contraction)
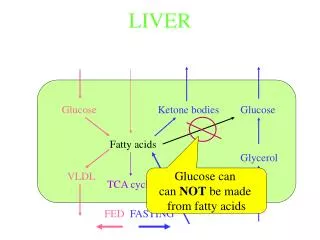
PROTEIN breakdown Muscle energy metabolism Dietary PROTEINS Gastrointestinal bacteria AMMONIA In the Liver UREA AMMONIA - Ruminal & Intestinal bacteria generate ammonia from proteins and other dietary nitrogen sources. - Ammonia also originates from protein breakdown and muscle energy metabolism. - Ammonia enters the portal circulation from the rumen & large intestine and is removed by the liver. - Urea cycle (in the liver) converts ammonia to urea. - High blood ammonia is toxic and can cause neurological signs
BLOOD AMMONIA MEASUREMENT - Ammonia is very labile - CAUSES OF INCREASED AMMONIA Hepatic dysfunction Portosystemic Shunts Congenital urea cycle enzyme deficiency (rare) Urea toxicosis (ruminants)
Sample handling: • Place blood into EDTA tube (in ice bath) • Separate plasma within 3 minutes (delayed separation of plasma can result in falsely increased values) • Plasma sample must be analysed within 30 minutes (delayed analysis can result in falsely decreased values) • Overload of fresh, easily hydrolizable plant proteins (alfalfa, clover) or urea can cause in ruminants hyperammonaemia.
DYE CLEARANCE TESTS • These tests are rarely used since the development of bile acid test • Measurement of dye in blood is very simple and may be useful when laboratories do not have the facilities to measure bile acids • Sulphobromophthalein (BSP) and indocyanine green (ICG) • Injected IV - cleared by the liver - dye level measured in the blood • High levels indicate hepatic dysfunction • BSP is no longer commercially available
OTHER TEST RESULTS THAT CAN INDICATE HEPATIC DISEASE • Anaemia • Haemorrhage due to coagulopathy (regenerative or non-regenerative) • Chronic disease • Microcytic ±hypochromic (functional iron abnormalities especially in PSS) • Coagulopathy • malabsorption of vitamin K due to cholestasis • synthesis of clotting factors • Hypoalbuminaemia ( production) • Hypoglycaemia ( gluconeogenesis) • Hypocholesterolaemia ( synthesis) • Hypercholesterolaemia (cholestasis causing cholesterol production and clearance of lipoproteins) • Hyperglobulinaemia (inflammation) • Decreased serum urea ( production by the liver) • Low urine specific gravity • ammonia excretion may inhibit renal concentrating mechanisms • urea synthesis renal medullary concentration gradient (medullary washout)