Download
1 / 1
40 likes | 193 Views
Translating Research into Practice (TRIP) Improving Sepsis Recognition and Treatment. What does the evidence say? Severe sepsis and septic shock continue to be major health care problems with a high mortality. One in four patients die and the incidence continues to increase.

E N D
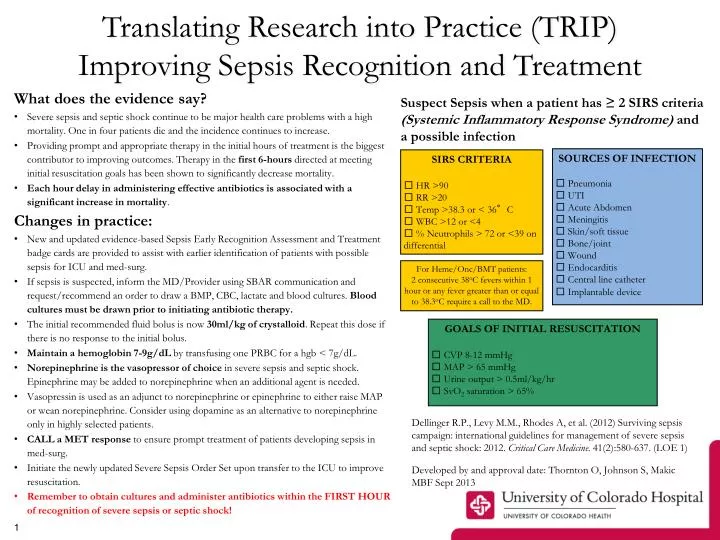
Translating Research into Practice (TRIP) Improving Sepsis Recognition and Treatment What does the evidence say? • Severe sepsis and septic shock continue to be major health care problems with a high mortality. One in four patients die and the incidence continues to increase. • Providing prompt and appropriate therapy in the initial hours of treatment is the biggest contributor to improving outcomes. Therapy in the first 6-hours directed at meeting initial resuscitation goals has been shown to significantly decrease mortality. • Each hour delay in administering effective antibiotics is associated with a significant increase in mortality. Changes in practice: • New and updated evidence-based Sepsis Early Recognition Assessment and Treatment badge cards are provided to assist with earlier identification of patients with possible sepsis for ICU and med-surg. • If sepsis is suspected, inform the MD/Provider using SBAR communication and request/recommend an order to draw a BMP, CBC, lactate and blood cultures. Blood cultures must be drawn prior to initiating antibiotic therapy. • The initial recommended fluid bolus is now 30ml/kg of crystalloid. Repeat this dose if there is no response to the initial bolus. • Maintain a hemoglobin 7-9g/dLby transfusing one PRBC for a hgb < 7g/dL. • Norepinephrine is the vasopressor of choice in severe sepsis and septic shock. Epinephrine may be added to norepinephrine when an additional agent is needed. • Vasopressin is used as an adjunct to norepinephrine or epinephrine to either raise MAP or wean norepinephrine. Consider using dopamine as an alternative to norepinephrine only in highly selected patients. • CALL a MET response to ensure prompt treatment of patients developing sepsis in med-surg. • Initiate the newly updated Severe Sepsis Order Set upon transfer to the ICU to improve resuscitation. • Remember to obtain cultures and administer antibiotics within the FIRST HOUR of recognition of severe sepsis or septic shock! Suspect Sepsis when a patient has ≥ 2 SIRS criteria (Systemic Inflammatory Response Syndrome) and a possible infection SOURCES OF INFECTION □ Pneumonia □ UTI □ Acute Abdomen □ Meningitis □ Skin/soft tissue □ Bone/joint □ Wound □ Endocarditis □ Central line catheter □ Implantable device SIRS CRITERIA □ HR >90 □ RR >20 □ Temp >38.3 or < 36°C □ WBC >12 or <4 □ % Neutrophils > 72 or <39 on differential For Heme/Onc/BMT patients: 2 consecutive 38oC fevers within 1 hour or any fever greater than or equal to 38.3oC require a call to the MD. GOALS OF INITIAL RESUSCITATION □ CVP 8-12 mmHg □ MAP > 65 mmHg □ Urine output > 0.5ml/kg/hr □ SvO2 saturation > 65% Dellinger R.P., Levy M.M., Rhodes A, et al. (2012) Surviving sepsis campaign: international guidelines for management of severe sepsis and septic shock: 2012.Critical Care Medicine. 41(2):580-637. (LOE 1) Developed by and approval date: Thornton O, Johnson S, Makic MBF Sept 2013