Download
1 / 44
850 likes | 1.61k Views
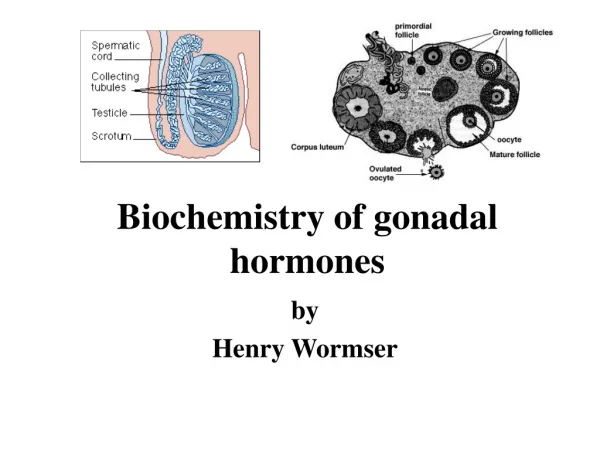
Biochemistry of Hormones. Biochemistry and Disorders of Hormones of the Hypothalamic and pituitary gland (hypothalamus. HORMONES OF THE ANTERIOR PITUITARY. The hormones secreted by the anterior lobe of the pituitary gland are: • Growth hormone, and

E N D
Biochemistry and Disorders of • Hormones of the Hypothalamic and • pituitary gland (hypothalamus
HORMONES OF THE ANTERIORPITUITARY • The hormones secreted by the anterior lobe of the pituitary gland are: • • Growth hormone, and • • Pituitary tropic hormones such as prolactin , gonadotropins FSH and LH, Thyrotropic hormones (TSH) and Adrenocorticotropic Hormone (ACTH).
GROWTH HORMONE (SOMATOTROPIN) • Chemistry: Growth hormone, also known as somatotropin, is a protein hormone of about 190 amino acids that is synthesized and secreted by cells called somatotrophs in the anterior pituitary. It is a major participant in control of several complex physiologic processes, including growth • and metabolism. Growth hormone is also of considerable interest as a drug used in both humans and animals.
Physiologic Effects of Growth Hormone • growth hormone has two distinct types of effects: • Direct effects are the result of growth hormone binding its receptor on target cells.Fat cells (adipocytes), for example, have growth hormone receptors, and growth hormone stimulates them to break down triglyceride and suppresses their ability to take up and accumulate circulating lipids. • Indirect effects: are mediated primarily by a insulin-like growth factor-1 (IGF-1), a hormone that is secreted from the liver and other tissues in response to growthhormone. • A majority of the growth promoting effects of growth hormone is actually due to IGF-1 acting on its target cells. IGF-1 also appears to be the key player in muscle growth. It stimulates amino acid uptake and protein synthesis in muscle and other tissues.:
Metabolic Effects of Growth hormone • Metabolic role: Growth hormone has a variety of effects on different tissues. The hormone acts slowly requiring from 1-2 hours to several days before its biological effects are detectable. This slow action and its stimulatory effects on RNA synthesis suggest that it is involved in protein synthesis. The hormone acts by binding to specific membrane receptors on its target cells
1. Protein synthesis: • Growth hormone brings about positive nitrogen balance by retaining nitrogen. It stimulates overall protein synthesis with an associated retention of phosphorus probably by increasing tubular reabsorption. Blood amino acid and urea level are decreased. It facilitates the entry of amino acids into the cell. In addition, growth hormone facilitates protein synthesis in muscle tissue by a mechanism independent of its ability to provide amino acids. Thus protein synthesis carries on even if the amino acid transport is blocked. • • Growth hormone increases DNA and RNA synthesis. • • It increases the synthesis of collagen.
2. Lipid metabolism: Growth hormone brings about lipolysis in a mild way by mobilising fatty acids from adipose tissue by activating the hormone sensitive triacylglycerol lipase. Thus it increases circulating free fatty acids. • 3. Carbohydrate metabolism: Growth hormone is a diabetogenic hormone, antagonises the effect of • insulin. Hypersecretion of GH can result in hyperglycaemia, poor sugar tolerance and glycosuria.
Growth hormone produces: • • Hyperglycaemia by increasing gluconeogenesis. • • It reduces insulin sensitivity and thereby decreases the hypoglycaemic effect of insulin. • • It brings about glycostatic effect, i.e. increases • liver glycogen. It can also increase muscle and cardiac glycogen level probably by reducing glycolysis.
4. Effect on growth of bones and cartilages: • Growth hormone when secreted in abnormally high concentration prolongs the growth of epiphyseal cartilages to cause overgrowth of long bones. • Acromegaly is found in adults. Hyposecretion causes 7stunted stature due to premature cessation of growth of the epiphyseal cartilages and consequently of long bones.
• The effect of growth hormone partly depends upon its calcium anabolic action. It promotes the retention of calcium and phosphate which helps in ossification and osteogenesis. • • It enhances the incorporation and hydroxylation of proline in the matrix collagen, incorporation of amines into glycosaminoglycans of cartilage, incorporation of sulphate into matrix proteoglycans like chondroitin sulphates, the synthesis of DNA and RNA in chondrocytes. • • The growth effects are mediated by a peptide called insulin-like growth factor I (IGF-I or somatomedin-C).
5. Prolactin action: Growth hormone has a sequence homology with prolactin. Growth hormone binds to membrane receptors for prolactin and stimulates the growth and enlargement of mammary glands. • 6. Ion or mineral metabolism: It is observed that the intestinal absorption of calcium is increased by GH, since the bone growth and development is stimulated by growth hormone. Growth hormone retains Na, Ca, K, Mg and PO4
Control of Growth Hormone Secretion • Production of growth hormone is modulated by many factors, including stress, exercise, nutrition, sleep and growth hormone itself. However, its primary controllers are two hypothalamic hormones and one hormone from the stomach:
Control of Growth Hormone Secretion • Growth hormone-releasing hormone (GHRH) is a hypothalamic peptide that stimulates both the synthesis and secretion of growth hormone. • · Somatostatin (SS) is a peptide produced by several tissues in the body, including the hypothalamus. Somatostatin inhibits growth hormone release in response to GHRH and to other stimulatory factors such as low blood glucose concentration. • · Ghrelin is a peptide hormone secreted from the stomach. Ghrelin binds to receptors on somatotrophs and potently stimulates secretion of growth hormone.
Control of Growth Hormone Secretion • Growth hormone secretion is also part of a negative feedback loop involving IGF-1. • High blood levels of IGF-1 lead to decreased secretion of growth hormone not only by directly suppressing the somatotroph, but by stimulating release of somatostatin from the hypothalamus. • Growth hormone also feeds back to inhibit GHRH secretion and probably has a direct (autocrine) inhibitory effect on secretion from the somatotroph. • Integration of all the factors that affect growth hormone synthesis and secretion lead to a pulsatile pattern of release. In children and young adults, the most intense period of growth hormone release is shortly after the onset of deep sleep.
Disease States • A deficiency state can result not only from a deficiency in production of the hormone, but in the target cell's response to the hormone. • Clinically, deficiency in growth hormone or receptor defects are known as growth retardation or dwarfism. The manifestation of growth hormone deficiency depends upon the age of onset of the disorder and can result from either heritable or acquired disease. • The effect of excessive secretion of growth hormone is also very dependent on the age of onset and is seen as two distinctive disorders:
Disease States • Gigantism is the result of excessive growth hormone secretion that begins in young children or adolescents. It is a very rare disorder, usually resulting from a tumor of somatotropes. • · Acromegaly results from excessive secretion of growth hormone in adults. The excessive growth hormone and IGF-1 also lead to metabolic derangements, including glucose intolerance.
PITUITARY TROPIC HORMONES • In addition to GH, anterior pituitary gland secretes some tropic hormones usually called as pituitary tropins.A tropin or tropic hormone is the one which influences the activities of other endocrine gland, principally those involved in stress and reproduction. These are carried by the blood to other target gland. the tropic hormones are usually subject to feedback inhibition at the pituitary or hypothalamic level by hormone product of the final target gland. Prolactin (mammotropin), TSH (or thyrotropin), FSH and LH (gonadotropins), ACTH (corticotropin) are the tropic hormones secreted by the pituitary gland.
A-Prolactin: PRL or Leuteotropic Hormone (LTH) • This is a monomeric simple protein (MW 23,000). It contains 199 amino acids with three –S–S–linkages. It is secreted by lactotroph α-cells of anterior pituitary and as already mentioned has sequence homology with growth hormone.
Metabolic role • • The main function of PRL is to stimulate mammary growth and the secretion of milk. By acting through specific glycoprotein receptors on plasma membrane of mammary gland cells, it stimulates mRNA synthesis. This ultimately leads to enlargement of breasts during pregnancy. This is called as mammotropic action. • • The synthesis of milk proteins such as lactalbumin,and casein takes place after parturition such an effect is called as lactogenic action. • •Estrogens, thyroid hormones and glucocorticoids increase the number of prolactin receptors on the mammary cell membrane. • • Progesterone has the opposite effect.
Control of Prolactin Secretion • In contrast to what is seen with all the other pituitary hormones, the hypothalamus suppresses prolactin secretion from the pituitary. • Dopamine serves as the major prolactininhibiting factor or brake on prolactin secretion. In addition to inhibition by dopamine, prolactin secretion is positively regulated by several hormones, including thyroid-releasing hormone, gonadotropinreleasing hormone and vasoactive intestinal polypeptide. • Estrogens provide a well-studied positive control over prolactin synthesis and secretion.
B. Thyrotropic Hormone or Thyroid Stimulating Hormone (TSH) • Thyroid-stimulating hormone, also known as thyrotropin, is secreted from cells in the anterior pituitary called thyrotrophs, finds its receptors on epithelial cells in the • thyroid gland, and stimulates that gland to synthesize and release thyroid hormones.TSH is a glycoprotein hormone composed of two subunits, which are non-covalently bound to one another. The alpha subunit of TSH is also present in two other pituitary glycoprotein hormones, follicle-stimulating hormone and luteinizing hormone. In other words, TSH is composed of alpha subunit bound to the TSH beta subunit, and TSH associates only with its own receptor. Free alpha and beta • subunits have essentially no biological activity.
Metabolic role • There are glycoprotein receptors on the thyroid cell membrane which bind to the receptor binding site on β-subunit of TSH. The complex then activates adenylate cyclase which catalyses the formation of c-AMP which acts as the second messenger for most TSH actions as follows:
Metabolic role • • The TSH stimulates the synthesis of thyroid hormones at all stages such as Iodine uptake, organification and coupling. • • It enhances the release of stored thyroid hormones. • • It increases DNA content, RNA and translation of • proteins, cell size. • • It stimulates glycolysis, TCA cycle, HMP and phospholipid synthesis. Stimulation of last two does not involve c-AMP. • • It activates adipose tissue lipase to enhance the release of fatty acids (lipolysis).
control of TSH secretion • The most important controller of TSH secretion is thyroid-releasing hormone. Secretion of thyroid-releasing hormone, and hence, TSH, is inhibited by high blood levels of thyroid hormones in a classical negative feedback loop. • .
C. Adrenocorticotropic Hormone (ACTH) or Corticotropin • Adrenocorticotropic hormone, stimulates the adrenal cortex by enhancing the conversion of cholesterol to pregnenolone. More specifically, it stimulates secretion of glucocorticoids such as cortisol, and has little control over secretion of aldosterone, the other major steroid hormone from the adrenal cortex. Another name for ACTH is corticotropin.
Metabolic role • ACTH increases the synthesis of corticosteroids by the adrenal cortex and also stimulates their release from the gland. Profound changes in the adrenal structure, chemical composition and enzymatic activity are observed as a response to ACTH. Total protein synthesis is found to be increased. Thus, ACTH produces both a tropic effect on steroid production and tropic effect on adrenal tissue. It is observed that ACTH has specific receptors on cells of fasciculata which increases c-AMP levels in the cell. This activation is calcium dependent. This results in DNA content and RNA is transcribed. This leads to proliferation of fasciculata cells and growth of adrenal cortex.
Metabolic role • 1• ACTH also stimulates the synthesis and secretion of glucocorticoids. • 2• ACTH is found to increase the transfer of cholesterol from plasma lipoproteins into the fasciculata cells. • 3•The ACTH induces rise in c-AMP, brings about phosphorylation and activation of cholesterolesterase. The enzyme action ultimately makes a large pool of free cholesterol. • •4 Corticotropin promotes the binding of cholesterol to mitochondrial cytochrome P450 required for hydroxylating cholesterol.
Metabolic role • 5•It activates the rate limiting enzyme for conversion of cholesterol to pregnenolone. • 6• It activates dehydrogenases of HMP to increase the conc. of NADPH required for hydroxylation. • 7• By activating adenylate cyclase of adipose tissue it increases intracellular c-AMP which in turn activates hormone sensitive lipase. This enzyme is involved in lipolysis which increases the level of free fatty acids.
Metabolic role • • It leads to increased ketogenesis and decreased RQ. • 8-• Direct effects on carbohydrate metabolism include: • • Lowering of blood glucose ↓; • • Increase in glucose tolerance; • • Deposition of glycogen in adipose tissue is increased, regarded as due to stimulation of insulin secretion. • 9-• It has MSH activity due to homology in amino acid sequence. • · Melanocyte-stimulating hormone (MSH): Known to control melanin pigmentation in the skin of most vertebrates.
Control of ACTH • ACTH is secreted from the anterior pituitary in response to corticotropin-releasing hormone from the hypothalamus. Corticotropin-releasing hormone is secreted in response to many types of stress, which makes sense in view of the "stress management" functions of glucocorticoids. • Corticotropin-releasing hormone itself is inhibited by glucocorticoids, making it part of a classical negative feedback loop.
D. Pituitary Gonadotropins • These tropic hormones influence the function and • maturation of the testes and ovary and are of two types: • • Follicle Stimulating Hormone (FSH) • • Luteinising Hormone (LH) • Both of them are glycoproteins with sialic acid, hexose and hexosamine as the carbohydrate moiety (16%). Molecular weight of FSH is 25000 and that of LH is 40000
Metabolic Role of FSH • It brings about its action by specific receptor binding and c-AMP. • In females: • • It promotes follicular growth • • Prepares the Graafian follicle for the action of LH and • • Enhances the release of estrogen induced by LH. • In males: • • It stimulates seminal tubule and testicular growth, • • Plays an important role in maturation of spermatozoa.
Role of FSH in Spermatogenesis • The conversion of primary spermatocytes into secondary spermatocytes in the seminiferous tubules is stimulated by FSH. In absence of FSH, spermatogenesis cannot proceed. However, FSH by itself cannot cause complete formation of spermatozoa. For its completion, testosterone is also required. Thus, FSH seems to initiate the proliferation process of spermatogenesis, and • testosterone is apparently necessary for final maturation of spermatozoa. Since the testosterone is secreted under the influence of LH, both FSH and LH must be secreted for normal spermatogenesis.
Metabolic Role of LH • This hormone is also known as interstitial cells stimulating hormone (ICSH).
Metabolic Role of LH In females • 1• It causes the final maturation of Graafian follicle and stimulates ovulation. • 2• Stimulates secretion of estrogen by the theca and granulosa cells. • 3• It helps in the formation and development of corpus luteum for luteinisation of cells. • 4• In conjunction with luteotropic hormone (LTH), it is concerned with the production of estrogen and progesterone by the corpus luteum. • 5• In the ovary it can stimulate the nongerminal elements, which contain the interstitial cells to produce the androgens, androstenedione, DHEA and testosterone.
Metabolic Role of LH • Action of LH in Ovulation : Ovulatory surge for LH • It is necessary for final follicular growth and ovulation. Without this hormone, even though large quantities of FSH are available, the follicle will not progress to the stage of ovulation. • LH acts synergistically with FSH to cause rapid swelling of the follicle shortly before ovulation. It is worth noting that especially large amount of LH called ovulatory surge is secreted by the pituitary during the day immediately preceding ovulation.
Metabolic Role of LH • Regulation of Testosterone Secretion by LH • Testosterone is produced by the interstitial cells of Leydig only when the testes are stimulated by LH from the pituitary gland, and the quantity of testosterone secreted varies approximately in proportion to the amount of LH available. Thus in males, LH stimulates the development and functional activity of Leydig cells (interstitial) and • consequently testicular androgen.
Control of Gonadotropin Secretion • The principle regulator of LH and FSH secretion is gonadotropin-releasing hormone or GnRH (also known as LH-releasing hormone). In a classical negative feedback loop, sex steroids inhibit secretion of GnRH and also appear to have direct negative effects on gonadotrophs.
Control of Gonadotropin Secretion • This regulatory loop leads to pulsatile secretion of LH and, to a much lesser extent, FSH. Numerous hormones influence GnRH secretion, and positive and negative control over GnRH and gonadotropin secretion is actually considerably more complex than described in the figure. For example, the gonads secrete at least two additional hormones - inhibin and activin , which selectively inhibit and activate FSH secretion from the pituitary.