Download
1 / 24
240 likes | 434 Views
Sex workers, policies and HIV Case from Central and Eastern Europe and Central Asia. Raminta Stuikyte 1 , Lucy Platt 2 , Nora Stojanovik 1,3 , Anna Alexandrova, Vania Dimitrievski 4 1 - Central and Eastern European Harm Reduction Network 2 – Imperial College, London

E N D
Sex workers, policies and HIV Case from Central and Eastern Europe and Central Asia Raminta Stuikyte1, Lucy Platt2, Nora Stojanovik1,3, Anna Alexandrova, Vania Dimitrievski4 1 - Central and Eastern European Harm Reduction Network 2 – Imperial College, London 3 – Drug Research Information and Training Center, Macedonia 4 – Macedonian Harm Reduction Network “Fostering Enabling Legal and Policy Environments for Sex Workers’ Health and Human Rights”, Johannesburg, South Africa, June 22-24, 2006
Report on 27 CEE/CA countries • Epidemiology • Sex work, HIV/STIs, drug use • Legislation and policies • Legal framework, violation of rights: police, media, clients, healthcare • Services for sex workers
Presentation focus • Sex work is the unforced sale of sexual services for money or goods between consenting adults • Individual sex work • Legislation and practices
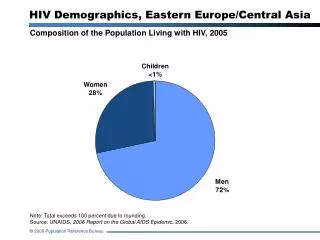
Central-Eastern Europe and Central Asia • Former Soviet Bloc • Population 400 m (UNDP, 2003) • HIV/AIDS: • Estimate 1.6 m (UNAIDS, 2005) • Fastest growing epidemics; mainly IDU, increasingly sexual transmission • Part of region with low prevalence • IDU: 3-6 m (UN Ref gr/IDU 2005; Russian Drug Control 2005) • Sex work: 800,000 (UNDP, 2004) • 1 in 4 Kazakh women at some point, Thomas 1997 • Sex work related HIV: data should be interpreted with caution; 0.1% in Russia in 2000 (in Moscow 15%); 0.8% in Ukraine in 1999; Albania almost all HIV cases in 2000 – related to trafficking for prostitution
Sex workers in the streets • Most vulnerable sex worker group • Age 20-30 (majority <25); up to 10% might be <18 • Usually have regular partners (20-66%) • High overlap of IDU and sex work esp Russia, Ukraine, Central Asia (up to 60-80%), some Baltics and Balkans • Condom use improving but inconsistent neither with paying clients, nor with regular non-paying partners; usually higher payment for not using condoms • Big part - not locals (from other cities or countries); or from ethnic minorities might have (il)legal residence status
Individual sex work:National regulation in CEE/CA • Direct prohibition • Absence of regulation • Explicit allowance
Direct prohibition • Half of countries (12 out of 27) • Criminal liability • Albania, Romania, • Administrative liability • Armenia, Belarus, BiH, Croatia, Lithuania*, Macedonia, Russia, Serbia and Montenegro, Turkmenistan, and Uzbekistan * Since July 2005, clients of sex workers are also punished according to administrative code in Lithuania. Ukraine eliminated criminalization of sex workers from the Criminal Code in 2006
Absence of regulation • No laws neither directly prohibiting nor explicitly allowing individual prostitution • Half of countries (13 out of 27) • Azerbaijan, Bulgaria, the Czech Republic, Estonia, Georgia, Kazakhstan, Kyrgyzstan, Moldova, Poland, Slovakia, Slovenia, Tajikistan and Ukraine
Sex work regulated • “Quasi-legal” individual prostitution in Hungary and Latvia • Sex work is allowed but the profession is not included in a list of officially registered professions • Many restrictions: • In designated “tolerance zones” only (however municipalities are not willing to define them) • mandatory HIV and STI testing, regular examination, any relevant information (STI status and treatment) is noted on the health care cards • Medical records are shared with the police
Regulation of individual prostitution, update 2006 RUS EST LAT LIT BEL POL UKR KAZ CZE HUN MDA ROM KGZ GEO BUL UZB ALB SLO TJK ARM TKM AZE SI HRV BIH FYM SRM Criminal offence Not regulated Administrative offence Allowed and regulated activity
Legislation in practice • Actual implementation of legislations is very different • Number of arrests vary in countries with sex work as an administrative offence
Sex work and pimping • Officially pimping and keeping brothels is regarded a bigger crime than sex work • But their registration and detection of crimes related to individual sex work and to pimping is on different levels No of detected cases in Belarus, 2003
Trafficking in Human Beings • Most countries have applied criminal punishment for trafficking in human beings • In practice only few countries are able or willing to adequately respond to the problem of trafficking. • Low number of convicted people involved in trafficking • Government officials do little to protect women from traffickers • Link between national laws prohibiting prostitution and a trafficked women’s fear of exposure as a sex worker
Human rights • Main reported issue – police harassment • Especially poorest sex workers in streets and highways and those injecting drug users • Forms: monthly “voluntary” (but in fact obligatory subotnik (esp Central Asia); rape (18% Moscow sex workers reported in 2002); • But there are good examples of police work • Other sources of violence and violation of rights: • Pimps • Mass media • Clients (80% of service providers reported violence) • Discrimination in healthcare settings • Overall negative public opinion
Sexual violence in different legal frameworks Sex workers respondents: Reported sexual violence against them, 2002 Administrative offence Not regulated Quasi-legal
Low self-organization and access to services • Estimated 8% of sex workers access HIV prevention in the region • The lowest coverage in the world • Harm reduction is of low scale and in harsh drug policy conditions • Social services, esp with work alternatives are not existing • Self-organizations of sex workers are reported from few countries (Ukraine, Lithuania, Hungary and Kyrgyzstan) • usually non-sex workers lead them • lack of information about them
Sex workers awareness • Low awareness about rights and possibilities to get services Awareness survey among sex workers 2004: what is legal liability for sex work? Two Kyrgyz cities; 2004; N=189 • Kyrgyzstan: 2/3 of sex workers didn’t know or had a wrong idea regarding punishment for sex work
Sex workers: issues (summary) • Risk behaviors, including IDU • Vulnerability • (Il)legal status • Stigma and discrimination • Low awareness of rights and self-organization • Low access to services • Bridge population for IDU concentrated epidemics?
Some conclusions • Current policies do not work and they often are not rationalized • Legislation changes does not mean better situation of sex workers • The main issue around sex workers’ rights – police practices • Sex workers’ role is low in decision making (policy and services)
What needs to be done for • Enabling policies and practices • Reducing stigma and discrimination • Provision of comprehensive, pragmatic services for those most in need • Ensuring that sex workers have the same rights as others • Sex workers to advocate for their own rights
What needs to be done(policymakers) • Greater commitment • Elimination of punishment for sex workers • Improving drug laws • Involving sex workers in policy and services
What needs to be done(healthcare decision makers) • Voluntary and confidential HIV testing • Harm reduction services • Migrants’ access to health care • Removing discriminative policies and procedures in health care delivery
What needs to be done(law enforcement) • Policies should be implemented to help stem harassment and abuse of sex workers by the police. • Regular training on issues related to HIV, drug use, and the legal and human rights of all individuals. • Police should also be expected to refer—but never in a coercive or threatening manner—sex workers and IDUs to programs, projects, and shelters where they can receive appropriate assistance.
What needs to be done • Expanding and diversifying services targeting sex workers and specific groups • better links with human rights organizations and activists to improve monitoring of human rights • Donors, especially foreign development agencies, need to base their response on the real situation on the ground and on scientific evidence • More research on HIV, sex workers and other vulnerable groups in CEE/CA • Analyzing effects of decriminalization of sex work