Download

1 / 27
270 likes | 343 Views
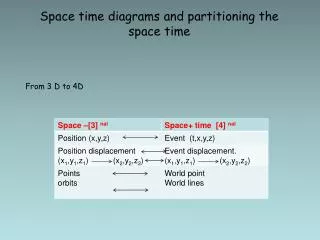
How Using Family Planning to Time and Space Pregnancies Reduces Mortality. Adrienne Allison, December 12, 2012. Family Planning to Time and Space Pregnancy.

E N D
How Using Family Planning to Time and Space Pregnancies Reduces Mortality Adrienne Allison, December 12, 2012
Family Planning to Time and Space Pregnancy • Using family planning to time and space pregnancies is the single most effective way to save lives and improve the health and well-being infants, children and mothers. • UNFPA, 2012
Outline of Presentation 1.Impact of FP Use on Infant, Child and Maternal Mortality 2.Impact of FP Use on Child Health 3. Family Planning Methods
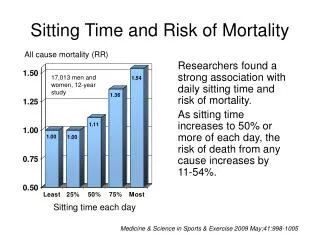
Impact of Birth Interval on Neonatal Mortality Rutstein 2005
Age of Mother Parity Spacing
Impact of Short Interpregnancy Intervals • Infants: increased risk of neonatal and perinatal mortality, low birth weight, preterm delivery • Children: mortality for children born 2 to 4 years apart is 75 per 1000 live births; for those born less than 2 years apart, it rises to 134 per 1000 • Mothers: higher risk of mortality, pre-eclampsia, ruptured membranes, anemia, high blood pressure • Infants whose mothers die are 3 to 10 times more likely to die before age one, compared to infants whose mothers live Rutstein, DHS, 2005 • Adolescent girls: pregnancy– related complications are the leading cause of mortality • Girls age 15 to 19 are twice as likely to die as women age 20 – 24 • Girls under 15 are 5 times more likely to die than those 20 - 24 • Infants of teenage girls are almost twice as likely to die as those born to women age 20 – 29SAVE, 2007, Guttmacher 2002
Longer Birth Intervals Decrease Stunting and Underweight Source for figure: Rustein, Shea, Effects of Birth Interval on Mortality and Health: Multivariate Cross-Country Analysis, MACRO International, Presentation at USAID, July 2000; Rutstein 2005; Dewey and Cohen, 2004.
The Need for Family Planning The risk: • Women who do not breastfed may become pregnant again as 25 days after giving birth • Without the protection of FP, 85% of sexually active women will become pregnant within the first year (USAID 2007)
Women Do Not Use Family Planning because of: • Lack of knowledge about FP methods • No easy access to health /FP services • Low quality health / FP services • Fears about side effects • Opposition from husbands, mothers-in- law • Cultural values
Contraceptive Methods • Most effective: Implants, IUD, Female Sterilization, Vasectomy • More effective: Injectables, LAM, Pills • Less effective: Male Condoms, Female Condoms, Fertility Awareness Methods (FAM) • Least effective: Withdrawal, Spermicides
Female Sterilization Ideally done within 48 hours after delivery May be performed immediately following delivery or during C/section If not performed within 1 week of delivery, delay for 4-6 weeks Highly effective, 99.5% comparable to vasectomy, implants, IUDs Follow local protocols for counseling clients and obtaining informed consent in advance Discuss during prenatal care
Male Sterilization: Vasectomy A safe, convenient, highly effective and simple form of contraception that is provided under local anesthesia in an out-patient setting Vasectomy is safer, simpler, less expensive and equally effective as female sterilization (tubal ligation) Highly effective in preventing pregnancy (99.6 to 99.8% effective) Not effective until after 3 months- requires a back-up contraceptive method during the first 12 weeks after a vasectomy
IUDs Can be inserted postpartum (immediately up to 48 hours after delivery) or after 4 to 6 weeks; Highly effective Effective immediately Long-term method (up to 12 years with Copper T 380A) Do not interfere with intercourse Do not affect breastfeeding, Few side effects 19
Combined Oral Contraception (COC) Start 3 weeks after delivery if not breastfeeding, 6 months after delivery if breastfeeding Highly effective when taken daily (0.1 – 0.5 pregnancies per 100 women during the first year of use) No pelvic exam or lab tests required to initiate use Can start even if menses has notreturned, but will need to use condoms or abstain for the first week of use Does not interfere with intercourse Client can stop use Can be provided by trained non-medical staff
Progestin-only contraceptives (pills, injectables, implants) No effect on breastfeeding, milk production or infant growth and development after infant is 6 weeks WHO recommends a delay of 6 weeks after childbirth before starting progestin-only methods to avoid newborn exposure to progestin If woman is using LAM, progestin-only is a good method to transition to at 6 months or when LAM criteria are no longer met (exclusive breastfeeding and menses not returned 21
Condoms When used consistently and correctly, male and female condoms are highly effective against pregnancy (97%) and STIs/HIV Can be used after childbirth (as soon as intercourse is resumed) 22
Lactational Amenorrhea Method (LAM) Protects from pregnancy if menses have not returned If Infant is less than six months old If mother is exclusively breastfeeding on demand (no more than 4 hours between feeds during the day; no more than 6 hours between feeds at night) Bonus effect - Immediate and exclusive breastfeeding for 6 months can reduce infant mortality by about 50%
Emergency Contraception Provides protection for up to 120 hours after unprotected intercourse, but should be taken immediately as effectiveness declines over 5 days If a woman is already pregnant, EC does not affect her pregnancy – she will remain pregnant Levonorgestrel, a progestogen hormone, works by stopping or disrupting ovulation, and may also prevent the egg and sperm from meeting After EC a mother needs immediate long term protection from pregnancy through a FP method
Female Sterilization Vasectomy IUD Implants Comparing effectiveness of methods Most effective How to make your method most effective Generally 2 or fewer pregnancies per 100 women in one year One-time procedures. Nothing to do or remember. Need repeat injections every 1 to 3 months Injectables Must take a pill each day Pills Must follow LAM instructions LAM About 15 pregnancies per 100 women in one year Must use every time you have sex; requires partner’s cooperation. Male Condoms Must use every time you have sex Diaphragm Must use every time you have sex; requires partner’s cooperation. Female Condom Must abstain or use condoms on fertile days; requires partner’s cooperation. Fertility Awareness-Based Methods About 30 pregnancies per 100 women in one year Must use every time you have sex Spermicides Least effective
Benefits of Using Family Planning Healthy newborns, infants, children, and women, and happy, stable families and communities.