Download
1 / 46
460 likes | 703 Views
Exercise and Altitude. Chapter 23 Brooks Ch 24 McArdle, Katch and Katch. Outline. Introduction to Altitude Acute altitude exposure Acclimatization Pulmonary Function Cardiovascular Function Muscle Nutrition Metabolism Athletics at Altitude Training Ergogenic aids.

E N D
Exercise and Altitude Chapter 23 Brooks Ch 24 McArdle, Katch and Katch
Outline • Introduction to Altitude • Acute altitude exposure • Acclimatization • Pulmonary Function • Cardiovascular Function • Muscle • Nutrition • Metabolism • Athletics at Altitude • Training • Ergogenic aids
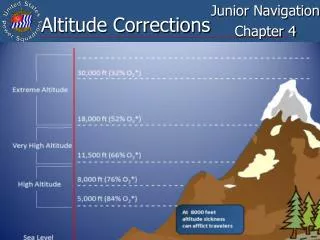
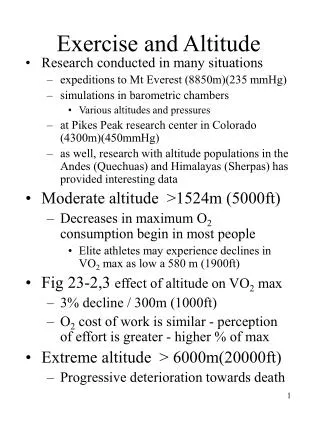
Exercise and Altitude • Research conducted in many places • expeditions to Mt Everest (8850m)(235 mmHg) • simulations in barometric chambers • Various altitudes and pressures • at Pikes Peak research center in Colorado (4300m)(450mmHg) • as well, research with altitude populations in the Andes (Quechuas) and Himalayas (Sherpas) has provided interesting data • Moderate altitude >1524m (5000ft) • Decreases in maximum O2 consumption begin in most people • Elite athletes may experience declines in VO2 max as low a 580 m (1900ft)
Exercise and Altitude • Fig 23-3,4effect of altitude on VO2max • 3% decline / 300m (1000ft) • O2 cost of work is similar - perception of effort is greater - higher % of max • Extreme altitude > 6000m(20000ft) • Progressive deterioration towards death
Acute Altitude Exposure • Sea Level 760mmHg(PIO2 159mmHg) • Fig 23-2 less O2 available • As barometric pressure decreases • Less air in given volume • Less O2 per volume of air • same % O2 as sea level (~ 21%)
Acute Altitude Exposure • Hypoxia - low levels of oxygen • Oxygen transport capacity decreases with increasing altitude, even with compensations outlined below • Table 23-1 Effects of Acute exposure • Increased resting and sub-maximal heart rate and ventilation • Increased catecholamine secretion • Decreased VO2 max • Few acute changes in blood, muscle or liver
Human Responses • With proper acclimatization humans can tolerate high altitudes • Table 23-2 - ability to adapt
Human Responses • Slow ascent to 5500m (18000ft) can be accomplished with few symptoms • Recommend 2 weeks to adjust to altitudes up to 2300m • Additional week for each 610 m up to 4600m • If ascent is rapid -AMS -acute mountain sickness - can occur within a few hours • Headache, nausea, irritability, weakness, poor appetite, vomiting, tachycardia, disturbed breathing • Above 3000m AMS is common • Those with a blunted breathing response are more susceptible • Slow ascent can reduce risk of AMS • Acclimatization hikes are important
Pulmonary Function • Ventilation increases further for first 2 weeks of exposure to a given high altitude • Hypoxia is the driving force • Bicarbonate is excreted by kidneys - increasing central and peripheral sensitivity for ventilation
Pulmonary Function • HVR - Hypoxic Ventilatory Response • fig 23-5 - ventilation during exercise • Important to maintain Alv and Art O2 • Which determines Max O2 utilization • Elite athletes - often have blunted HVR
Pulmonary Function • Fig 23-6 - O2 tensions at rest and exercise
Pulmonary Function • Fig 23-6 - O2 tensions at rest and exercise
Pulmonary Function • Observe decrease in PaO2 with intense exercise • May be pulmonary gas exchange causing diffusion limitation at altitude • Partial Pressure of O2 determines driving force • Fig 23-7b - same transit time - dec driving force (slope) at altitude
pH Changes and Ventilation • Higher ventilation decreases PCO2 • Blood becomes more alkaline • First Week • Decrease bicarbonate level in cerebrospinal fluid resulting from active transport and kidney excretion • helps to normalize pH • improves respiratory control at altitude • influence of bicarbonate release on pH is limited - at high altitude blood still alkaline • Fig 23-7 a - O2 Hb dissociation curve
3,000 m 5,500 m Brooks, Exercise Physiology 2005
pH Changes and Ventilation • Higher ventilation inc PaO2 but also cause shift of curve to left • tighter bond between Hb and O2 • require lower PO2 to release O2 at tissues • Bicarb excretion shifts curve back to right • Helps unloading of O2 at tissues • increased content of 2,3-DPG in rbc’s causes curve to shift further to the right • Advantageous only to 5000m - then impairs ability to pick up O2 at the lungs
Cardiovascular Adjustments • Acute submaximal exercise • HR inc; SV ~ same; Q inc; VO2 inc • Acclimatized submaximal exercise • HR still high; SV dec, • Q dec 20-25% (after 1-2 weeks); • VO2 ~same • MAP - Mean Arterial BP - gradually increases with exposure • Due to inc systemic resistance and vascular resistance in muscle • inc blood viscosity and catecholamines • Above 3000m EPO stimulates Hb and Hct - requires several weeks • Time reduced with adequate energy, protein and iron intake
Acclimatization • Rate Pressure Product - work load on heart (HR * Systolic BP) • Shown to inc 100% in some individuals with exercise at 3000m and above • Poses significant challenge to the heart • Lungs -PAP-pulmonary Arterial P • Inc with altitude due to • sympathetic stimulation • Inc size of sm ms in pulmonary arterioles • Implicated in HAPE (high altitude pulmonary edema) • Brain - hypoxemia - vasodilation • Implicated in HACE (cerebral edema) • Hypocapnea causes vasoconstriction in brain which can reduce vasodilation
Muscle Acclimatization • During exercise • Sub-maximal blood flow decreases by about 20-25% • Due to inc Nor Epinephrine and decreased Q • O2 delivery maintained - through increased O2 content in blood • Inc myoglobin, buffering capacity, aerobic enzymes CS (small change) • Enhances tissue oxygenation and acid base balance • Oxidative capacity - no change?? • Altitude native populations - low mitochondrial volume • Activity limited by pulmonary ventilation and arterial O2 content • Even unfit are thought to have sufficient muscle Oxidative capacity at altitude • Endurance capacity increases with acclimatization • with no change in VO2 max
Nutrition and Energetics • Weight loss and muscles atrophy are common average 100-200 g/day - • dehydration, energy deficit, increased activity and BMR • High carbohydrate diet recommended > 60% • Exercise Energetics • Lactate paradox - fig 23-9 • Blood lactate is higher at given power output with acute exposure compared to sea level and acclimatization • Paradox is that there is no change in VO2 max with acclimatization
Nutrition and Energetics • Fig 23-10 • research suggests that acclimatization results in Dec Ep, (Nor Ep stays high) • Reduced glycogen mobilization • Working ms oxidizes more of its own lactate - inc dependence on bld glucose
Fuel Metabolism • Carbohydrates - thought to be preferred fuel - higher yield of ATP/O2 • CHO has very limited storage • Hypoglycemia and liver glycogen depletion common at altitude • Reduced with high carbohydrate diet • Fat and Protein • Increased fat catabolism at altitude if diet is inadequate • Gluconeogenesis - loss of muscle mass also occurs with low CHO intake • Working muscle shown to prefer CHO at altitude • Use of protein for gluconeogenesis has detrimental impact on long term exercise/work potential
Athletics at Altitude • Table 23-3 -Mexico City Olympics (1968) • ~ 2240m (7350ft) • Improvements in short duration, high intensity events • Reduced gravity and wind resistance • Decreased endurance performance • longer than 800m • Athletes benefit from 1-12 weeks of acclimatization • Problem - reduced absolute training intensity at altitude-even if same relative % • Can not train as hard - detraining effect • Further - do not see improvements in sea level performance (reduction) • Reduced bld volume, buffering capacity, inc ventilation (more work)
Live High - Train Low • Combine benefits of sedentary adaptations to altitude with maximal training stimulus near sea level • Increased capacity to compete at moderate altitude • Recent research has also illustrated an increased capacity for exercise at sea level with live high-train low • Levine, Stray-Gunderson and Chapman • Fig 21.6 (Brooks) • VO2 Max and Running Endurance improved • 3000m performance improved (elite) • Only some subjects were ‘responders’- significant EPO production with altitude
Live High - Train Low • Either live at 2200-3500m and drive down every day to train (<1200m) • This altitude found to stimulate rbc production, but to not cause AMS symptoms in athletes • Or sleep in hypoxic tent with reduced oxygen tension (14%O2 - PIO2 106mmHg) • Stimulates adaptation while you sleep
Ergogenic Aids and Altitude • Significant use of EPO and synthetic analog of EPO at Salt Lake City Olympics • Several athletes stripped of their medals in cross country skiing • Used darbepoietin - novel erythropoiesis stimulating protein • Developed for the treatment of of chronic anemia in patients on renal dialysis • Longer half life than EPO, needs to be taken less frequently, but also stays in system longer making detection easier • Currently, limits of absolute levels of Hb and/or Hct are in place • 50% and 17g/dl (males)(varies with organization) • Proposals for indirect analysis of soluble transferrin receptors and serum erythropoietin which can be done in minutes