Download
1 / 41
410 likes | 644 Views
Treating Nicotine Dependency. Paul Zemann Public Health - Seattle & King County Tobacco Prevention Program 401 5 th Ave, Suite 900 Seattle, WA 98104 paul.zemann@kingcounty.gov. Overview. Importance of nicotine treatment for clients Three-link chain of addiction

E N D
Treating Nicotine Dependency Paul Zemann Public Health - Seattle & King County Tobacco Prevention Program 401 5th Ave, Suite 900 Seattle, WA 98104 paul.zemann@kingcounty.gov
Overview • Importance of nicotine treatment for clients • Three-link chain of addiction • What nicotine dependency treatment look like “THE 5 A’s and 5 R’s • Preventing Relapse
Be aware that: • Tobacco dependence is chronic • Tobacco users may have other addictions • The physical and psychological environment is part of the message • Community resources are available • We have interventions that work
Systematic Approach • Client-centered • Specific to your audience • Evidence-based • Integrated into your practice
Patients Want to Quit • Documented interest in quitting among clients across all treatment modalities • Standard treatment approaches work (NRT plus behavioral counseling) • Promise of emerging new drugs • Patients are already in a secure, supportive environment ideal for nicotine cessation
An Unfair Share of Mortality Number of Deaths (thousands) Est. 200,000 per year for mentally ill and SA AIDS Alcohol Motor Homicide Drug Suicide Smoking Vehicle Induced Source: CDC
Why Don’t They Just Quit? + No Cessation Help
Three-Link Chain 1. Biological addiction to nicotine • Feeling of pleasure, decrease in anxiety • Lasting chemical changes in brain • Quitting produces withdrawal symptoms 2. Psychological addiction to smoking • Triggered by other behaviors • Self-medication
How is nicotine the same/different from other addictive drugs? • 85+% who use nicotine, use daily • 10% of cocaine/alcohol users • Withdrawal not life-threatening • Can be for alcohol • Most severe consequences delayed
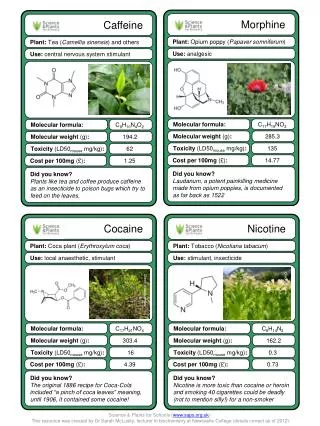
Tobacco Delivered Nicotine – a Chemical Cocktail • Acetaldehyde : synergistic addictive effects • Ammonia: increase speed and efficiency of nicotine absorption • Leuvenalic acid, chocolate and menthol: may increase ease of inhalation and deep lung absorption • Menthol: may also provide a cue for Pavlovian conditioning • Physical engineeringby particle physicists results in more rapid and efficient absorption of nicotine and toxins • Glycerin: can form particles to enable deep lung exposure • Ventilation holesmay increase free nicotine fraction
Three-Link Chain (cont’d) 3. Cultural support for smoking addiction • Friends who smoke • Activities that involve smoking PLUS: Limited access to treatment
Cessation Tools • Counseling • Doubles quit rates • More counseling (time, modes, different people) increases quit success • Brief – 3-10 minutes at a time • Nicotine Replacement Therapy (NRT) • With counseling, can double quit rates • Available free from Public Health • Reduces withdrawal symptoms
ASK • Ask clients at screening or when appropriate if they smoke
ADVISE Urge every tobacco user to quit • Clear: “One of the best things you can do for your health is to quit smoking. I can help you.” • Strong: “As your case manager, I need you to know that quitting smoking is one of the most important things you can do for your health.” • Personalized: Tie tobacco use to current health issues, relationships, or economic stress
ASSESS Ask every tobacco user about quitting • Examples: • “On a scale of 1 to 5, how ready do you feel to quit?” • “Have you thought about quitting in the next 30 days?” • If the patient is ready to quit in the next 30 days provide assistance • If the patient is not ready to quit provide a motivational intervention (5R’s)
ASSIST Help the ready client make a quit plan • Set a quit date in 30 days • Plan to tell friends • Anticipate challenges • Plan to remove tobacco products • Recommend NRT use
Behavioral Change • Stress - Deep Breathing, understanding of nicotine's role in generating stress, delay, call a friend • Weight gain – Increase activity level, don’t substitute food for smokes, NRT • Triggers – Anticipate and cope • Increase Self Efficacy – positive “self talk”
ARRANGE Plan a time to follow-up after quit-date • Congratulate success • Address challenges • Assess NRT use
Motivational Interviewing Is • Starting where client is • Understanding client’s frame of reference • Knowing choice to change is client’s • Exploring options with client • Finding and reinforcing the client’s motivation to change
Nicotine Replacement Therapy • NRT increases quit success (patch/counseling doubles rate) • Safe, FDA approved, available OTC • Reduces most withdrawal symptoms so quitter can comfortably break the habit • Eliminates the reinforcing effect of nicotine as administered through smoking
Appear within hours, last up to weeks Withdrawal Symptoms • Depressed mood • Insomnia • Irritability • Frustration • Anger • Anxiety • Difficulty concentrating • Restlessness • Decreased heart rate • Increased appetite or weight gain
What NRT Does Not Do • Without behavioral change/counseling, does not increase quit rates • NRT does not replace smoking • Clients will still want to smoke • Does not provide bolus effect (nicotine rush)
Currently available products • Over-the-counter • Patch – available from Public Health • Gum • Lozenge • Prescription • Oral Inhaler • Nasal Inhaler • Bupropion (Zyban®, Wellburtrin®) – non-nicotine • Varenicline (Chantix®) – non-nicotine
Smoking and NRT • Client should stop smoking on quit date • “Slipping” will happen, and is not harmful • If client continues to smoke after starting patch • Assess if they are really ready to quit • Address triggers for smoking • Nausea, dizziness, vomiting
Quitting the Three Link Chain NRT Posters Groups Activities Behavioral Counseling + Cessation Help
Relapse Is Common • Tobacco dependence is chronic • Cycle through relapse and remission • 5 to 7 times not uncommon • 7% long-term success quit on own • Relapse not a failure—for patient or you
Nicotine withdrawal discomfort Negative emotions Use of drugs & alcohol Stressful situations Traumatic events Lack of social support Social pressure Level of addiction or dependence Interpersonal conflict Loneliness Depression Weight gain Common Causes of Relapse
Preventing Relapse • Congratulate success • Address challenges • Review benefits of quitting • Offer encouragement • Refer to services, Washington Tobacco Quit Line
Remember “Quitting smoking is the easiest thing in the world to do, I’ve done it a thousand times!” Mark Twain