Download
1 / 36
880 likes | 2.78k Views
Pathophysiology of Hypertension. Jianzhong Sheng MD, PhD. Department of Pathophysiology, School of Medicine. Regulation of ABP:. ■ Maintaining B.P. is important to ensure a steady blood flow (perfusion) to tissues. ■ BP is regulated neurally through centers in medulla oblongata:

E N D
Pathophysiology of Hypertension Jianzhong Sheng MD, PhD Department of Pathophysiology, School of Medicine
Regulation of ABP: ■Maintaining B.P. is important to ensure a steady blood flow (perfusion) to tissues. ■BP is regulated neurally through centers in medulla oblongata: 1. Vasomotor Center (V.M.C.), or (pressor area): Sympathetic fibers. 2. Cardiac Inhibitory Center (C.I.C.), or (depressor area): Parasympathetic fibers (vagus).
cardiac control centers in medulla oblongata Regulation of ABP(continued) 1. Cardiacaccelerator center (V.M.C) 2. Cardiacinhibitory center (C.I.C) Sympathetic n. fibers Parasympathetic n. fibers • Regulatory mechanisms depend on: • a.Fast acting reflexes: • Concerned by controlling CO (SV, HR), & PR. • b.Long-term mechanism: • Concerned mainly by regulating the blood volume.
Regulation of Arterial Blood Pressure Regulation of Cardiac Output Regulation of Peripheral Resistance Regulation of Blood Volume
Classification of hypertension • Essential hypertension • Secondary hypertension
Some of the factors involved in the control of blood pressure that affect the basic equation: blood pressue = cadiac output x peripheral resistence. Excess sodium intake Reduced nephron number Stress Endothlium derived factors Obesity Genetic alteration Decreased filtration surface Hyper- insulinaemia Renin angiotensin excess Renal sodium retention Cell membrane alteration Sympathetic nervous over activity Fluid volume Venous constriction Heart Contractability Structural hypertrophy Functional constriction Preload Blood pressure = Cardiac output X Peripheral resistance Hypertension = Increased CO and/or Increased PR Autoregulation
A. Regulation of CO: ■A fast acting mechanism. ■CO regulation depends on the regulation of: a. Stroke volume, & b. Heart rate Regulation of Arterial Blood Pressure
A. Regulation of the CO: Mean arterial pressure Cardiac output = Stroke volume X Heart rate End Contraction diastolic strength volume (EDV) Stretch Sympathetic n Parasympathetic n Frank - Starling
Regulation of Arterial Blood Pressure B. Regulation of Peripheral Resistance
B. Regulation of Peripheral Resistance (PR): ■A fast acting mechanism. ■Controlled by 3 mechanisms: 1. Intrinsic. 2. Extrinsic. 3. Paracrine.
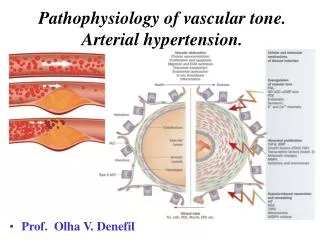
Intrinsic mechanism: Blood vessel tone
Extrinsic mechanism is controlled through several reflex mechanisms, most important: 1. Baroreceptors reflex. 2. Chemoreceptors reflex.
1. Baroreceptors reflex: ■ Baroreceptors are receptors found in carotid sinus & aortic arch. ■ Are stimulated by changes in BP. BP + Baroreceptors = V.M.C ++ C.I.C = Sympathetic + Parasympathetic Slowing of SA node ( HR) & CO Vasodilatation & TPR
2. Chemoreceptors reflex: ■Chemoreceptors are receptors found in carotid & aortic bodies. ■Are stimulated by chemical changes in blood mainly hypoxia ( O2), hypercapnia ( CO2), & pH changes. Haemorrhage BP Hypoxia + Chemoreceptors = C.I.C ++ V.M.C + Sympathetic = Parasympathetic + Adrenal medulla HR Vasoconstriction & TPR
3. Other Vasomotor Reflexes: 1.Atrial stretch receptor reflex: Venous Return ++ atrial stretch receptors reflex vasodilatation & BP. 2.Thermoreceptors: (in skin/or hypothalamus) Exposure to heat vasodilatation. Exposure to cold vasoconstriction. 3. Pulmonary receptors: Lung inflation vasoconstriction.
4. Hormonal Agents: ■NA vasoconstriction. ■A vasoconstriction (except in sk. ms.). ■ Angiotensin II vasoconstriction. ■ Vasopressin vasoconstriction.
Regulation of Arterial Blood Pressure C. Regulation of Blood Volume
Regulation of Blood Volume: ■A long-term regulatory mechanism. ■Mainly renal: 1. Renin-Angiotensin System. 2. Anti-diuretic hormone (ADH), or vasopressin. 3. Low-pressure volume receptors.
1. Renin-Angiotensin System: ■Most important mechanism for Na+ retention in order to maintain the blood volume. ■Any drop of renal blood flow &/or Na+, will stimulate volume receptors found in juxtaglomerular apparatus of the kidneys to secrete Renin which will act on the Angiotensin System leading to production of aldosterone.
Renin-Angiotensin System: renal blood flow &/or Na+ ++ Juxtaglomerular apparatus of kidneys (considered volume receptors) Renin Angiotensinogen Angiotensin I Converting enzymes (Lungs) Angiotensin II (powerful vasoconstrictor) Angiotensin III (powerful vasoconstrictor) Adrenal cortex Corticosterone Aldosterone • N.B. Aldosterone is the main regulator of Na+ retention.
2. Anti-diuretic hormone (ADH), or vasopressin: ■Hypovolemia & dehydration will stimulate the osmoreceptors in the hypothalamus, which will lead to release of ADH from posterior pituitary gland. ■ADH will cause water reabsorption at kidney tubules.
3. Low-pressure volume receptors: ■Atrial natriuritic peptide (ANP) hormone, is secreted from the wall of right atrium to regulate Na+ excretion in order to maintain blood volume.
Proposed mechanism of pressure natriuresis. Increased renal perfusion pressure Increased pressure and flow vasa recta Increased renal interstitial pressure Washout of medullary solute gradient Deep nephrons Decreased sodium resorption in proximal tubule Possible thin descending limb Possible thick ascending limb Superficial nephrons Decreased sodium resorption in proximal tubule Possible thick ascending limb
Fig. 3 : Low birth weight and impaired renal development Acquired glomerular sclerosis Reduction in FSA (Filtration surface area) Systemic/glomerular hypertension
Central venous volume Venous tone Na+ ingestion (-) [Ca 2+ ]i [Na +]i Venous smooth muscle Na+(+Cl + H2O) Plasma volume retention Kidneys (-) (-) ADH Adolsterone Renin ANP Ouabain [Na +]i [Ca 2+ ]i platelets Na+ excretion Endothelium [Na +]i [Ca 2+ ]i Arterial smooth Muscle [Na +]i [Ca 2+ ]i NO Sympathetic neurons [Na +]i [Ca 2+ ]i (-) Cardiovascular reflex activity Catecholamine Re-uptake Catecholamine release (-) (+) Blood pressure Arterial tone
Angiotensinogen Macula densa signal Renal arteriolar pressure Renin Angiotensin I Renal nerve activity Converting enzyme Angiotensin II Angiotension III Angiotensinase A Arenal cortex Kideney Intestine CNS Vascular Smooth muscle Heart Peripheal Nervous system Adrenergic facilitation Contracctility Aldosterone Sympathetic discharge Sodium and Water reabsorption Distal nephron reabsorption Thirst Salt appetite Vasopression release Vasoconstriction Maintain or increase ECFV Total periphral resistance Cardiac output
High renin (Dry vasoconstriction) Low renin (wet vasoconstriction) Pathophysiologic difference Arterioles Peripheral resistance Aldosterone Plasma volume Cardiac output Haematocrit Blood urea Blood viscosity Tissue perfusion Postural hypotension Higher High Low Low High High Low Yes High Low to High High High Low Low High NO Clinical examples High renin essential hypertesion Renovascular and malignant hypertension Low renin essential hypertesion Primary aldosteronism Vascular sequelae (+) Stroke (-) (+) Heart attack (-) (+) Renal damage (-) (+) Retinopathy encephalopathy (-) Treatments (+) Converting enzyme inhibitors (-) (+) Beta blockers (-) (-) Calcium channel blockers (+) (-) Diuretics (+) (-) Alpha blockers (+)
Genetics Stress Resetting of cadiovascular centers Increased sympathetic outflow Cadiovascular centers Renin-angiotension system Increased arterial pressure Increased vascular resistance Endothelium derived relaxing factors Endothelium and platelet derived mitogens Vascular hypertrophy Endothelium derived contracting factors
Sympathetic nervous system Renin- angiotensin Other (genetic) Episodic hypertension Norepinephrine angiotensin II Peritubular capillary pressure Peritubular capillary flow Capillary damage tubulointerstitial injury Ischaemia NO Adenosine Ang II RSNA Capillary injury Capillary rarefaction Renal vascular Resistance Tubuloglomerular feed back Pressure natriuresis NaCl excretion Salt-dependent hypertension
Na-K ATPase (co-transport) Cell Na Na fluxes K fluxes Depolarisation Ca binding Ca ATPase others Cell Ca Contractility Na retention Na-H antiport (Na-Li counter T) Cell pH Growth
Na+ / H + exchange Renal proximal tubule cells Vascular smooth muscle cells Na reabsorption Cell Na and pH Cai2+ Vascular volume expansion Vascular tone Growth Vascular wall thickness Peripheral resistance Hypertension
Acetycholine Endothelial cell Ca2+ Calmodulin NO synthase Arginine +O2 Citrulline + NO NO Smooth muscle cell Fe Guanyate Cyclase GTP cGMP Relaxation
Dyslipidaemia Lipolysis Obsity + Androgen increased abdominal fat Release of free fatty acids Decreased hepatic insulin extraction Increased pancreatic insulin secretion Peripheral insulin resistance Type 2 diabetes mellitus X Hyperinsulinaemia Increased sympathetic nervous activity Sodium retention Vascular hypertrophy Attenuated vasodilation Hypertension
Normal human insulin Obesity or hypertension insulin Sympathetic activation Vasodilation Potentiated sympathetic activation Impaired depressor action Increased Blood pressure Decreased Blood pressure Impaired Depressor action Augmented Pressure action No increase in blood pressure Elevated blood pressure