Download
1 / 1

E N D
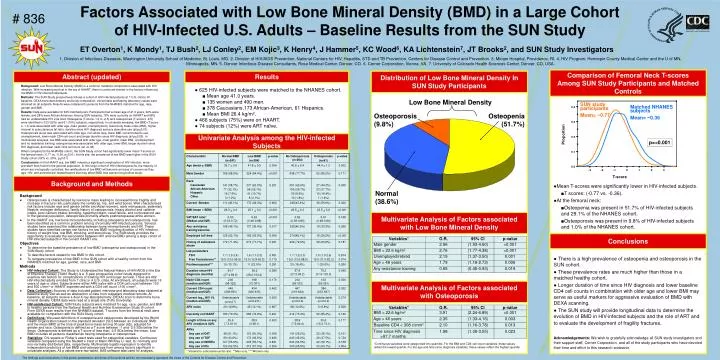
Background Osteoporosis is characterized by low bone mass leading to increased bone fragility and increase in fracture risk, particularly the vertebrae, hip, and wrist bones. Well characterized risk factors include race and gender (white and Asian women), early menopause, sedentary lifestyle, estrogen deficiency, family history of osteoporosis, heavy alcohol and caffeine intake, poor calcium intake, smoking, hyperthyroidism, renal failure, and corticosteroid use. In the general population, osteoporosis primarily affects postmenopausal white women. In the HAART era, low bone mineral density, including osteopenia and osteoporosis, has been identified as a common problem among chronically HIV-infected persons. Several studies have examined the relationship between bone mineral density and HIV. These studies have identified certain risk factors for low BMD including duration of HIV infection, history of weight loss, low BMI, smoking, and steroid use. The SUN study provides the opportunity to evaluate the association between HIV and low BMD among a large cohort of HIV-infected subjects in the current HAART era. Objectives To determine the baseline prevalence of low BMD (osteopenia and osteoporosis) in the SUN Study cohort. To describe factors related to low BMD in this cohort. To compare prevalence of low BMD in the SUN cohort with a healthy cohort from the NHANES matched for age, gender, race, and BMI. Methods HIV-infected Cohort: The Study to Understand the Natural History of HIV/AIDS in the Era of Effective Therapy (‘SUN’ Study) is a 5-year prospective cohort study designed to examine risk factors for complications of treating HIV and longer survival. There are 682 HIV-infected adults enrolled from 7 clinic in 4 U.S. cities. At enrollment, all subjects were 18 years of age or older. Subjects were either ARV-naïve with a CD4 cell count between 100 and 500 c/mm3 or HAART experienced with a CD4 cell count >100 c/mm3. Data Collection: Sources of data included patient interview and laboratory data obtained at baseline study visit as well as abstraction of data from outpatient medical records. At baseline, all subjects receive a dual X-ray absorptiometry (DEXA) scan to determine bone mineral density. DEXA data were read at a single site (Tufts University). HIV-uninfected Cohort: SUN Study subjects were matched for age, race, gender, and BMI to healthy persons from the National Health and Nutrition Examination Study III cohort. From DEXA scan results from the NHANES dataset, T scores from the femoral neck were available for comparison with the SUN Study cohort. Definitions: We used definitions of osteopenia and osteoporosis developed by the World Health Organization based on the standard deviation (SD) between an individuals' BMD and the mean BMD at the time of peak bone mass among 30 year olds, adjusted for gender and race. Osteopenia is defined as a T score between -1 and -2.5 SDs below the mean. Osteoporosis is defined as a T score of less than -2.5 SDs below the mean. Low BMD includes all persons classified as having osteopenia or osteoporosis. Statistics: Chi-square or Fisher’s exact tests used for categorical variables. Continuous variables compared using the Student’s t-test or Mann-Whitney U test, for normally and non-normally distributed data, respectively. Multivariate logistic regression to identify independent predictors of low BMD and osteoporosis from among factors significant in univariate analyses. All p values were two-tailed. SAS software was used for analysis. Factors Associated with Low Bone Mineral Density (BMD) in a Large Cohort of HIV-Infected U.S. Adults – Baseline Results from the SUN Study # 836 ET Overton1, K Mondy1, TJ Bush2, LJ Conley2, EM Kojic3, K Henry4, J Hammer5, KC Wood6, KA Lichtenstein7, JT Brooks2, and SUN Study Investigators 1. Division of Infectious Diseases, Washington University School of Medicine, St. Louis, MO. 2. Division of HIV/AIDS Prevention, National Centers for HIV, Hepatitis, STD and TB Prevention, Centers for Disease Control and Prevention. 3. Miriam Hospital, Providence, RI. 4. HIV Program, Hennepin County Medical Center and the U of MN, Minneapolis, MN. 5. Denver Infectious Disease Consultants, Rose Medical Center, Denver, CO. 6. Cerner Corporation, Vienna, VA. 7. University of Colorado Health Sciences Center, Denver, CO, USA. Comparison of Femoral Neck T-scores Among SUN Study Participants and Matched Controls Abstract (updated) Results Distribution of Low Bone Mineral Density In SUN Study Participants Distribution of Low Bone Mineral Density In SUN Study Participants Background: Low Bone Mineral Density (BMD) is a common metabolic complication associated with HIV infection. With increasing survival in the era of HAART, there is continued interest in the factors influencing low BMD in HIV-infected individuals. Methods: The SUN Study prospectively follows a cohort of HIV-infected patients at 7 U.S. clinics. At baseline, DEXA bone densitometry and body composition, clinical data and fasting laboratory values were obtained on all subjects. Results were compared to persons from the NHANES matched for age, race, gender and BMI. Results: Data were available for 625 matched pairs. Participants had a mean age of 41.0 years, 22% were female, and 28% were African American. Among SUN subjects, 78% were currently on HAART and 58% had an undetectable HIV viral load. Osteopenia (T-score -1.0 to -2.5) and osteoporosis (T-score ≤ -2.5) were identified in 323 (52%) and 61 (10%) subjects, respectively. In univariate analyses, low BMD (T-score ≤ -1.0) was associated with older age, male gender, unemployment, lower body mass index (BMI), higher visceral to subcutaneous fat ratio, duration since HIV diagnosis and any stavudine use (all p<0.01). Osteoporosis alone was associated with older age, non-white race, lower BMI, current tobacco use, unemployment, lower nadir CD4 cell count and longer duration since HIV diagnosis (all p<0.05). In multivariate analyses, low BMD was associated with older age, male gender, lower BMI, unemployment and no resistance training; osteoporosis was associated with older age, lower BMI, longer duration since HIV diagnosis, and lower nadir CD4 cell count (all <0.05). When compared to the NHANES cohort, the SUN Study cohort had significantly lower mean T-scores at the femoral neck (-0.77 vs. -0.36, p<0.01). At this site, the prevalence of low BMD was higher in the SUN Study cohort (52% vs. 29%, p<0.01). Conclusions: In the HAART era, low BMD remains a significant complication of HIV infection, more prevalent than found in the general population. In this large cohort of HIV-infected persons, the majority of whom are virologically controlled, the ramifications of low BMD will become an issue of concern as they age. HIV- and antiretroviral-related factors that may affect BMD loss warrant longitudinal study. • 625 HIV-infected subjects were matched to the NHANES cohort. • Mean age 41.0 years. • 135 women and 490 men. • 378 Caucasians,173 African-American, 61 Hispanics. • Mean BMI 26.4 kg/m2. • 466 subjects (75%) were on HAART. • 74 subjects (12%) were ART naïve. Low Bone Mineral Density SUN study participants Mean= −0.77 Matched NHANES subjects Mean= −0.36 Osteoporosis (9.8%) Osteopenia (51.7%) Proportion Univariate Analysis among the HIV-infected Subjects p=<0.001 T-score Background and Methods • Mean T-scores were significantly lower in HIV-infected subjects. • T scores: (-0.77 vs. -0.36). • At the femoral neck: • Osteopenia was present in 51.7% of HIV-infected subjects and 29.1% of the NHANES cohort. • Osteoporosis was present in 9.8% of HIV-infected subjects and 1.0% of the NHANES cohort. Normal (38.6%) Multivariate Analysis of Factors associated with Low Bone Mineral Density Conclusions • There is a high prevalence of osteopenia and osteoporosis in the SUN cohort. • These prevalence rates are much higher than those in a matched healthy cohort. • Longer duration of time since HIV diagnosis and lower baseline CD4 cell counts in combination with older age and lower BMI may serve as useful markers for aggressive evaluation of BMD with DEXA scanning. • The SUN study will provide longitudinal data to determine the evolution of BMD in HIV-infected subjects and the role of ART and to evaluate the development of fragility fractures. Acknowledgements: We wish to gratefully acknowledge all SUN study investigators and their support staff, Cerner Corporation, and all of the study participants who have devoted their time and effort to this research endeavor. Multivariate Analysis of Factors associated with Osteoporosis *Continuous variables were categorized into quartiles. For the BMI and CD4 cell count variables, these values reflect the lowest quartile. For the age and time since diagnosis variables, these values reflect the highest quartile * Visceral to subcutaneous fat ratio. **Men only. *** Women only. The findings and conclusions in this poster presentation are those of the authors and do not necessarily represent the views of the Centers for Disease Control and Prevention.






















