Download

1 / 30
300 likes | 415 Views
£3bn Budget. 3,000,000 Patients. 81,000 Staff. 15,000 Beds. ~2000 GP Practices. 135 Hospitals. 22 LHBs. 15 Trusts. 3 Regions. 1 Assembly. Cardiff and Vale Gwent Swansea Bro Mor NW Wales Conwy and Den NE Wales Ponty and Rhon Carmarthenshire N Glamorgan

E N D
£3bn Budget 3,000,000 Patients 81,000 Staff 15,000 Beds ~2000 GP Practices 135 Hospitals 22 LHBs 15 Trusts 3 Regions 1 Assembly
Cardiff and Vale Gwent Swansea Bro Mor NW Wales Conwy and Den NE Wales Ponty and Rhon Carmarthenshire N Glamorgan Pembs and Der Velindre Welsh Ambulance Powys Ceredigion Revenue Secondary Care Budget
Legacy iSoft/ ‘Green screen’ Myrddyn PIMS PMS CWS/ I Soft I Soft/ PIMS Pembs PAS Velindre WAS BSC
Legacy • In the south, mid and west of Wales the tradition is local development Typically: • PAS • Clinical work station • Departmental systems • Some primary care (GP system) links Usually developed in single Trust, two were later shared with neighbours
Legacy • North Wales has commercial systems of varying vintages with more limited in house development capacity Almost all Trusts use national systems from the corporate era: • Radiology • Pathology • Pharmacy
Our Health Informatics People • Reflect the legacy • Variations in capacity, resource levels and skill sets across Wales • Many Trusts have strong in house teams • Successful implementations • Invaluable knowledge of clinical processes • Excellent relationships with local clinicians • We are know seeking to exploit this resource • Two pieces of strategic work • Deployment and utilisation • Professional development
Staff Deployment and Utilisation Strategy • Four phase production of strategy • First two phases completed • Best practice model derived • Service wide survey and gap analysis against model completed • CEOs have approved phase 2 report and authorised phases 3 and 4 • Stage 3 - appraisal of options to improve the utilisation of workforce and meet future requirements • Stage 4 - recommended option, strategy and implementation plan (completion October 2006)
Professional Development Strategy Professional Development Programme Talent Management Standards Education Training CPD Identity & Community • Recruitment • Retention • Career progression • Workforce planning • Leadership development • A4C/KSF • Succession planning • HI National • Occupational • Standards • UKCHIP • Other professional • standards • Bursary scheme • Vocational schemes • Modular E&T products • CPD initiatives • Community of practice • Body of knowledge • Professional bodies • UK HI professional • development bodies • Branding & marketing
Local ‘Readiness’ • Programme inheritance 1% of NHS resources • NHS Wales target 2%, Wanless 4% • Initially emphasis therefore on strengthening generic weaknesses • So in first three years of programme • £41m invested – 65% through local organisations • 15 project managers and 19 support staff employed locally • Networks improved (150 extra sites)
Local ‘Readiness’ • Over 8000 ‘access devices’ deployed • Microsoft enterprise agreement - 35,000 desk tops • Data cleansing and quality • 100 staff deployed locally • Over 780,000 records processed by July 2006 • Duplicates down 4.6% to 1.4% • Missing NHS numbers down 31% to 13% • Foundation skills – European Computer Driving License • 13,000 registered • 25,000 modules passed
Local ‘Readiness’ • Future readiness • Derived from CMiS, IHR and Service Improvement Projects • National work needed e.g. common clinical terminologies / coding • But cannot continue to operate at 65% local allocation • Higher proportion will be national • Local requirements subject to business cases and benefit realisation
Engaging with NHS Wales • This has been a top priority for the IHC Programme • Stakeholder and communications strategy • Some traditional approaches • But key has been ‘hearts and minds’ through face to face relationships e.g. • Every organisation visited by Implementation Director at three monthly intervals • Programme funded project managers in every Trust • Residential stakeholder events e.g. National Architecture Event • Stakeholder assurance groups for key projects • Programme Director attendance CEOs meetings • Key strategic thinking explained and tested locally • Position achieved: we are working ‘in common' is the default
Engaging with NHS Wales • This activity must now ‘ramp up’ further • We must ‘reach down’ further into organisations • Must make use of local internal communication arrangements • Deploy professional communication techniques • Use our health care professionals to engage with professional communities • These activities are resource intensive but a critical success factor in technology supported change
Current Position • Overall • We have an underinvested and fragmented legacy position (systems and staff) • But … • Programme regarded as moving to new phase and changing pace • Delivery of strategic partner and CMiS foundation phase seen as key • Engagement approach continues to be commended – Trust level and events • Increasing sense of ‘corporateness’, partnership and realism • IHC Programme is increasingly expected to give leadership & direction
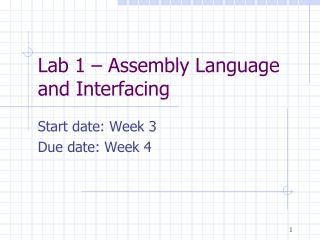
Mrs Jones’ Journey Information in silos Primary care Record 1 consultation & referral Follow-up Follow-up Home nursing Record 2 Symptomatic care Hospice Record 3 Specialist palliative care Hospital unit Record 4 specialist consultation Follow-up Diagnostic unit Record 5 investigations second treatment Radio/chemotherapy centre Record 6 pre-operative treatment Surgical centre Record 7 Surgery Multidisciplinary team Record 8 First case conference Second case conference Time
Patient Journey with New Information Services Information in silos Primary care Record 1 consultation & referral Follow-up Follow-up Home nursing Record 2 Symptomatic care Hospice Record 3 Specialist palliative care Hospital unit Record 4 specialist consultation Follow-up Diagnostic unit Record 5 investigations second treatment Radio/chemotherapy centre Record 6 pre-operative treatment Surgical centre Record 7 Surgery Multidisciplinary team Record 8 First case conference Second case conference New information services Time
What have we done so far? • Network improvements • Improving access to technology • IT skills • Electronic library • Reducing duplicate records • Service Improvement Projects • My Health On-Line • Diabetes Monitoring • Individual Health Record – ‘Out of Hours’ • Transfer of Care Communication
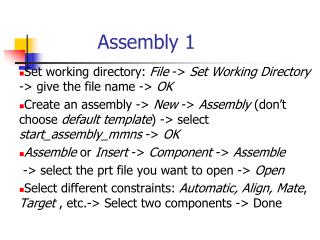
Organising to Deliver Informing Healthcare Programme Sub-programme Project NHS business change resources, benefits management Projects Business assurance Stakeholder assurance Technical assurance NADB Business change National architecture Projects Service improvement projects Projects Programme board Executive team Programme review meetings Individual Health Record Corporate programme resources
IHC Strategic Partner • Why do we need one? • NHS Wales does not yet have the required collective internal capacity & capability to deliver the programme • There is a need for significant flexibility in constructing teams (skill share, scarce resources) • To scale up and deploy existing services and support new developments • Create momentum as quickly as possible. The success of this relationship and a combined ability to craft change is of equal importance to the more formal, contractual obligations
IHC Strategic Partner • Some of the things the partner will do for us … • Joint working with NHS Wales and other countries • Capability and capacity • Hosting services • Management of the catalogue – a restricted choice of common services only • Technical development expertise • Continuity support – legacy
IHC Strategic Partner • Some of the things they will not do for us … • Overall design • Final choice of systems • Stakeholder engagement • Implementation plan
Supplier Engagement • To date, open dialogue prior to procurement • Do suppliers fully understand IHC’s approach? • How do suppliers view working with IHC? • How will suppliers approach securing the market capability and capacity to support the Programme? • Do suppliers actually have the capability to support the IHC design principles? • Is the scope of the programme commercially attractive to suppliers?
Approach • Supplier Day: March 2006 • Phase 1 workshops: May - July 2006 • Phase 2 workshops: July - September 2006 • Intellect UK Briefing: May 2006 • Concept Viability: September 2006 • Issue OJEU Notice: Jan - march • 7 months of constant dialogue with the market place • 20 workshops within supplier community • 50 hours of open dialogue outside workshops • 50+ responses to Prior Information Notice (PIN)
Findings • Incremental approach of IHC is much welcomed • Catalogue approach best approach to meeting service requirements • Strict governance around management of the catalogue is required, but flexible enough to meet service requirements • Broad support for service orientated architecture approach – helping to leverage existing and new capabilities • Delivery using service orientated architecture approach is relatively untried in healthcare • Strong governance will be needed to balance IHC & the partnership
Sustained investment determined by service change priorities Sustained investment ahead of service change INCREASING PATIENT BENEFITS Investment Decisions IHC AIMS Shared view of care Individual Health Record Core foundation services World class infra- structure Catalogue of information services required to deliver safe, effective and efficient healthcare Enabling change Regional plans, clinical futures, Delivering integrated services, care close to home
Sustained investment determined by service change priorities Sustained investment ahead of service change Timescale for Designed for Life (Yrs) 0 3 6 9 Implementation Strategy and Benefits Realisation IHC AIMS Shared view of care Individual Health Record Core foundation services World class infra- structure Catalogue of information services required to deliver safe, effective and efficient healthcare Enabling change Regional plans, clinical futures, Delivering integrated services, care close to home
Sustained investment determined by service change priorities Sustained investment ahead of service change Timescale for Designed for Life (Yrs) 0 3 6 9 Implementation Strategy and Benefits Realisation IHC AIMS Shared view of care IHR in emergency care IHR for long term conditions Clinical correspondence via portal MHOL patient access Patient Record Service
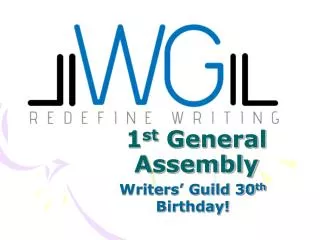
Sustained investment ahead of service change Timescale for Designed for Life (Yrs) 0 3 6 9 INCREASING PATIENT BENEFITS Implementation Strategy and Benefits Realisation IHC AIMS World class infra- structure Pt & Carer Emp. Portal services Data storage & Processing facilities Registration & Audit Authority Patient ID Service (PMI) - home countries & RoI Local and National Messaging Services Legacy Integration Services Patient Authentication for internet access to summary record Mobile and fixed network connectivity for all clinicians Sustained investment determined by service change priorities Scheduling Ordering & Results Rep. Referrals/Discharge Imaging Pathology National email service Medicines Management Video conferencing, Access to IT, Knowledge & Learning – All Existing Services Cancer Information – Existing Service (CANISC) Readiness – Data Quality, Info Gov. – Existing Services
Sustained investment determined by service change priorities Sustained investment ahead of service change Timescale for Designed for Life (Yrs) 0 3 6 9 INCREASING PATIENT BENEFITS Implementation Strategy and Benefits Realisation IHC AIMS Regional Plans Clinical Futures Enabling change Bro Morgannwg Care close to home – (e.g. National Tele-Dermatology & National Minor Injuries Service) Project 2009 Patient Safety Integrated Care Pathways Decision Support