Download
1 / 37
380 likes | 498 Views
Meaningful Use of Electronic Health Records. Tammy Geltmaker, RN, BSN, MHA EHR Consulting Manager November 17, 2010. Highlights. Eligible Professionals (EP) Financial Incentives Meaningful Use (MU) Stage One Measures Kentucky Resources. American Recovery and Reinvestment Act (ARRA).

E N D
Meaningful Use of Electronic Health Records Tammy Geltmaker, RN, BSN, MHA EHR Consulting Manager November 17, 2010
Highlights • Eligible Professionals (EP) • Financial Incentives • Meaningful Use (MU) • Stage One Measures • Kentucky Resources 11/17/2010
American Recovery and Reinvestment Act (ARRA) • A Massive Stimulus for Health Information Technology (HIT) Adoption & Health Information Exchange (HIE) Expansion • Appropriations for HIT • Appropriations for HIE • New incentives for adoption • Community Health Centers • Broadband and Telehealth 11/17/2010
Eligible Professional (EP) • Eligible Providers- Medicare * Defined: Section 1861(r) Physician Definition 11/17/2010
Eligible Professional (EP)- Medicare Advantage (MA) • MA Eligible Professionals (EPs) • Must furnish, on average, at least 20 hours/week of patient-care services and . . . • Be employed by the qualifying MA organization Or . . . • Must be employed by, or a partner of, an entity contracting with the qualifying MA organization furnishing at least 80 percent of the entity’s Medicare patient care services to enrollees of the qualifying MA organization • Qualifying MA-Affiliated Eligible Hospitals • Will be paid under the Medicare Fee-for-service EHR incentive program 11/17/2010
Eligible Professional (EP) • Patient volume requirements for Medicaid incentives 11/17/2010
Registration Process • Register through the EHR Incentive Program Web site • Be enrolled in Medicare FFS, MA, or Medicaid (FFS or managed care) • Have a National Provider Identifier (NPI) • Use certified EHR technology to demonstrate MU • Medicaid providers may adopt, implement, or upgrade in their first year • All Medicare providers and Medicaid eligible hospitals must be enrolled in Provider Enrollment, Chain and Ownership System (PECOS) 11/17/2010
Registration: Medicaid • States will connect to the EHR Incentive Program Web site to verify provider eligibility and prevent duplicate payments • States will ask providers for additional information to make accurate and timely payments • Patient Volume • Licensure • A/I/U or Meaningful Use • Certified EHR Technology 11/17/2010
Financial Incentives • Includes financial incentives for health care providers who attain “meaningful use” with their EHR systems. • Medicare: Up to $44,000 per provider over five years • Medicaid: Up to $63,750 per provider over six years 11/17/2010
Medicare Incentives 11/17/2010
Medicare Incentives (Cont’d) • Pays 75% of “allowed charges” based on claims submitted to Medicare • MA providers qualify for the Medicare incentives using MA claims instead of part B claims 11/17/2010
Medicaid Incentives 11/17/2010
Medicaid Incentives (Cont’d) • EPs may receive up to 85 percent of the net average allowable costs for certified EHR technology, including support and training, up to a maximum level of $63,750. • Pediatricians must have a Medicaid patient volume of at least 20%. 11/17/2010
Medicaid Only: Adopt/Implement/Upgrade (A/I/U) • First participation year only for Medicaid providers • Adopted-Acquired and Installed • e.g., Evidence of installation prior to incentive • Implemented–Commended Utilization of • e.g., Staff training, data entry of patient demographic information into EHR • Upgraded–Expanded • e.g., Upgraded to certified EHR technology or added new functionality to meet the definition of certified EHR technology • Must use certified EHR technology • No EHR reporting period 11/17/2010
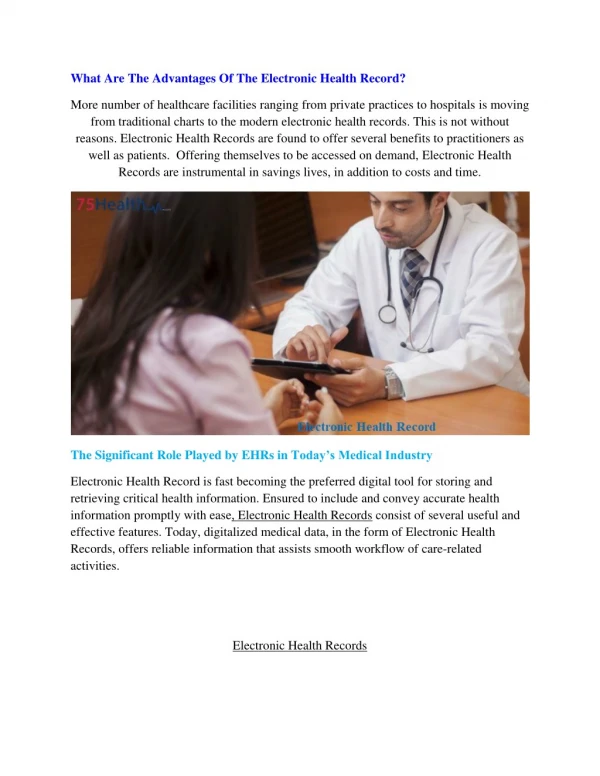
Meaningful Use Definition • Meaningful use is defined as . . . • Use of a certified EHR in a meaningful manner (ex: e-prescribing) • Use of certified EHR technology for electronic exchange of health information • Use of certified EHR technology to submit clinical quality and other measures 11/17/2010
Meaningful Use Stages * Stages 2 and 3 will be defined in future CMS rulemaking 11/17/2010
Meaningful Use Stages 11/17/2010
Stage One Priorities • Electronically capture information in a coded format • Use electronic information to track key clinical conditions • Implement clinical decision support tools to facilitate disease and medication management • Report clinical quality measures and public health information 11/17/2010
Stage One Measures • HIT functionality measures • Reported by attestation • Clinical quality measures • Reported by attestation for 2011 • Electronic submission to CMS for 2012 11/17/2010
HIT Functionality Measures • EPs must report on 20 of 25 MU objectives with associated measures • Core set of 15 • Menu set of 10 • An EP must successfully meet the measure for each objective in the core set and all but five in the menu set • Some MU objectives are not applicable to every provider’s clinical practice. In this case, the EP would be excluded from having to meet that measure. • e.g., Dentists who do not perform immunizations and chiropractors who do not have prescribing authority 11/17/2010
Meaningful Use: Core Set Objectives EPs –15 Core Objectives • Computerized physician order entry (CPOE) • E-Prescribing (eRx) • Report ambulatory clinical quality measures to CMS/States • Implement one clinical decision support rule • Provide patients with an electronic copy of their health information, upon request • Provide clinical summaries for patients for each office visit • Drug-drug and drug-allergy interaction checks • Record demographics • Maintain an up-to-date problem list of current and active diagnoses • Maintain active medication list • Maintain active medication allergy list • Record and chart changes in vital signs • Record smoking status for patients 13 years or older • Capability to exchange key clinical information among providers of care and patient-authorized entities electronically • Protect electronic health information 11/17/2010
Meaningful Use: Menu Set Objectives EPs – 10 Menu Objectives • Drug-formulary checks • Incorporate clinical lab test results as structured data • Generate lists of patients by specific conditions • Send reminders to patients per patient preference for preventive/follow up care • Provide patients with timely electronic access to their health information • Use certified EHR technology to identify patient-specific education resources and provide to patient, if appropriate • Medication reconciliation • Summary of care record for each transition of care/referrals • Capability to submit electronic data to immunization registries/systems* • Capability to provide electronic syndromic surveillance data to public health agencies* *At least 1 public health objective must be selected 11/17/2010
Clinical Quality Measures • Ambulatory setting report on all (3) of the core measures as applicable for their patients • Inquiry regarding tobacco use • Blood pressure measurement • Adult weight screening and follow-up • Alternate core measures if denominator is zero • Preventative care and screening • Influenza immunization for patients ≥50 years old • Weight assessment and counseling for children and adolescents • Childhood Immunization status 11/17/2010
Clinical Quality Measures (Cont’d) • Second required measure set for each EP to submit information on three additional measures from at list of 38 clinical qualitymeasures • Specifications for the measures are published in the final rule • In sum, EPs must report on 6 total measures: 3 required core measures (substituting alternate core measures where necessary) and 3 additional measures 11/17/2010
Meaningful Use Reporting Period • First Year Incentive Qualifications • Any continuous 90-day period within a payment year in which an EP successfully demonstrates meaningful use of certified EHR • First opportunity to start demonstrating meaningful use is January 1, 2011 • “Attestation methodology” proposed in 2011 • Electronic Reporting starting in 2012 • Subsequent years reporting period • Entire 12 months (calendar year for EP) in the respective year 11/17/2010
Certification Process/Bodies • Temporary Process • Currently three certifying bodies • Certification Commission for Health Information Technology (CCHIT), Drummond Group Inc., InfoGard Laboratories Inc. • Certification process has begun • ONC is posting the certified EHR applications on its site • To obtain Medicare incentive dollars, must be a CERTIFIED EHR system 11/17/2010
Certification Process/Bodies (Cont’d) • Permanent Process • Accreditation of bodies expected to be completed through private entities with guidance from National Institute of Standards and Technology (NIST) • Expected timeframe for first bodies under permanent program to be accredited by January 2012 11/17/2010
Certified EHR Technology • Two Types of Certification of EHR Technology • Complete EHR • EHR must certify all requirements to certify as Complete EHR • Certified EHR Module • “..any service, component, or combination thereof that can meet the requirements of at least one certification criterion adopted by the Secretary” 11/17/2010
Penalties • No incentive money available for implementation • Medicare cuts begin • 2015=1% • 2016=2% • 2017=3% • Evaluation of adoption rate in 2018 • No Medicaid cuts associated with non-adoption 11/17/2010
EHR Incentive Programs Milestone Timeline 11/17/2010
Comparison of Medicare and Medicaid Programs 11/17/2010
Participation in Other Incentive Programs 11/17/2010
Kentucky’s Efforts Kentucky Health Information Exchange • In 2005, Senate Bill 2 created the Kentucky eHealth Network (KeHN) Board to oversee the development, implementation, and operation of a statewide e-health network. • Kentucky also received a Medicaid Transformation Grant to develop the foundational components for a statewide health information exchange, the Kentucky Health Information Exchange (KHIE), to be completed by the second quarter of 2010. 11/17/2010
Kentucky’s Efforts (Cont’d) Regional Extension Centers • Providing basic resources for assisting practices with adopting EHRs and achieving meaningful use • Emphasis placed on • small practices (fewer than10 prescribers; physicians, PAs, ARNPs) • community health centers • rural clinicians that work with critical access hospitals • practices and clinics that serve the underserved 11/17/2010
Additional Assistance Kentucky Medical Association • More information regarding “EHR Planning Available for KMA Member Practices” on the KMA Web site https://www.kyma.org/content.asp 11/17/2010
Questions ? Tammy Geltmaker RN, BSN, MHA (502) 454-5112, ext. 2201 tgeltmaker@hce.org For further details regarding information found in this presentation, please visit http://www.cms.gov/EHRIncentivePrograms 11/17/2010