Download
1 / 27
270 likes | 492 Views
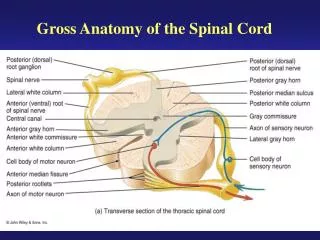
Spinal Immobilization Harmful or Helpful?. Jason Hoffman EMT-P, CC EMT-P. Objectives:. Discuss the problem of using mechanism of injury (MOI) as the primary indicator for spinal immobilization. Discuss the harmful outcomes of spinal immobilization.

E N D
Spinal ImmobilizationHarmful or Helpful? Jason Hoffman EMT-P, CC EMT-P
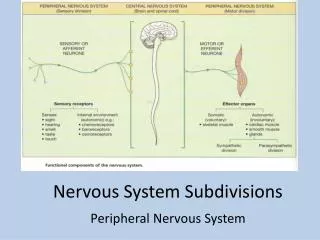
Objectives: • Discuss the problem of using mechanism of injury (MOI) as the primary indicator for spinal immobilization. • Discuss the harmful outcomes of spinal immobilization. • Discuss a sub-set of trauma patients who should NOT be immobilized. • Discuss appropriate spine injury assessment as. Look at an “ideal” protocol.
“I am just following protocols.” “When in doubt…” One of the most common “treatments” done by EMS everyday, whether the patient needs it or not. “This is just precautionary.”“Better safe then sorry.”“We don’t diagnose in the field.”
Mechanism of Injury (MOI) • MOI Video
NYS EMT-B Protocol • Suspected Spinal Injuries (Not Meeting Major Trauma Criteria) • This protocol is for awake and stable adult and pediatric patients NOT meeting the Major Trauma Criteria (Protocol T – 6). • Spine injury should be suspected if blunt mechanism of injury is present and should be treated if one or more of the following criteria is present:
NYS EMT-B Protocol (con’t) IMMOBILIZATION CRITERIA • 1. Altered Mental Status for any reason, including possible intoxication from alcohol or drugs (GCS <15 or AVPU other than A). • 2. Complaint of neck and/or spine pain or tenderness. • 3. Weakness, tingling, or numbness of the trunk or extremities at any time since the injury. • 4. Deformity of the spine not present prior to this incident. • 5. Distracting injury or circumstances (i.e. anything producing an unreliable physical exam or history). • High risk mechanisms of injury associated with unstable spinal injuries include, but are not limited to: • Axial load (i.e. diving injury, spearing tackle)• High speed motorized vehicle crashes or rollover • Falls greater than standing height • IF THERE IS ANY DOUBT, SUSPECT THAT A SPINE INJURY IS PRESENT!
A CLIMBER fell 1,000ft from the top of a mountain – and walked away. Adam Potter, 35, quickly became the subject of a helicopter rescue mission – but when they found him he was standing up, reading a map.
Why do we Immobilize? • In theory– “to prevent secondary cord injuries.” • Further manipulation makes any spinal injury potential worse or more severe. • Manipulation of unstable fractures may cause a cord injury. • IN REALITY: • Tradtion • Dogma • Fear of Litigation • ER criticism • There is no evidence immobilization helps……at all!
Journal of Trauma. 2010 Jan; 68; discussion 120-1. • Name of Article– Spine Immobilization in penetrating trauma: more harm then good? • Immobilization is “a tradition that started decades ago” said Dr. Demetriades. “There was never any scientific evidence that it works.” • The author reports first responders would have to immobilize 1,032 patients before potentially benefiting one person. While it only took immobilizing 66 patients before potentially contributing to a death.
Boston GlobeInjured woman drowns while strapped to a backboard. • Virginia Yates, 64, of Rockingham, Vt., was stepping on a dock when she slipped Tuesday, injured her head. • “She didn't want to go in the ambulance. She didn't want to be rescued” • ``Why would you take a 64-year-old lady that's got a little bump on the head and a strained ankle and strap her into a situation where if there was an accident, she couldn't get out?"
Potentially harmful side effects of Spinal Immobilization. • Pain • Increased pain which leads to patient needing sometimes unnecessary X-Rays/CT. • Anxiety • Cause we need our patients to be more anxious. • Aspiration • Lying supine, your risk of aspiration increases. • Head injury patients tend to vomit. • Increased ICP • Respiratory Compromise • 15-20% reduction in respiratory capacity. • Skin ulcers • Heels, buttocks, shoulders. • Time delay • On scene, in ER.
Patient Assessment What’s not wrong? What’s wrong?
What’s wrong? What’s not wrong? -Clear Mental Status -Clear of New Symptoms -Clear Physical Exam A “CLEAR” Spine Assessment means that there is no spine injury and no need for spinal immobilization.
“Clear Mental Status” • Reliable patient • No significant distracting injury. • Not intoxicated. • Cooperative.
“Clear of New Symptoms” • No new complaint of significant neck or back pain. • No new complaint of distal numbness or weakness. • Any positive findings during this exam means you should treat for a spinal injury.
“Clear Physical Exam” • Distal motor and sensory exam is intact. • Finger or wrist abduction/extension against resistance. • Dorsiflexion or Plantarflexion of foot or big toe. • No tingling or numbness • Intact sensory perception
Ok…. So all this talk about not immobilizing. Who SHOULD we immobilize? • MOI for a spinal injury is present AND… • Pt is unconscious/not alert. • Patient has significant neck/back pain with tenderness. • Neuro-defecits. • Significant multi-system trauma. • BAD TRAUMA!
Wake County EMSNorth Carolina • Protocols are written orders from our Medical Director that tell our personnel what they can do to treat patients. The Medical Director of the Wake County EMS System has entrusted our Advanced Life Support personnel with progressive, standing order-based protocols. • The Wake County EMS System has some of the most aggressive protocols in the U.S. • Our protocols are reviewed and revised on an annual basis and must be approved by the Wake County Peer Review Committee and the North Carolina Office of EMS prior to implementation.
What a Spinal Immobilization Protocol should look like… • Wake County Protocol 83
Other More Effective Spinal Immobilization Equipment • Vacuum Mattresses • Highly effective • More comfortable • Keeps patients immobilized, warm, and comfortable. • Weight is more evenly distributed. • Many Studies published as to the benefits in using vacuum mattresses as opposed to LBB.
Summary • MOI is a very poor predictor of spinal injury. • A proper Physical Assessment can rule out most spinal injuries. • Most EMS protocols call for unnecessary spinal immobilization. • Spinal Immobilization has harmful consequences. • A different approach along with different tools will have more beneficial results for patients in need of spinal immobilization.