Download
1 / 21
210 likes | 214 Views
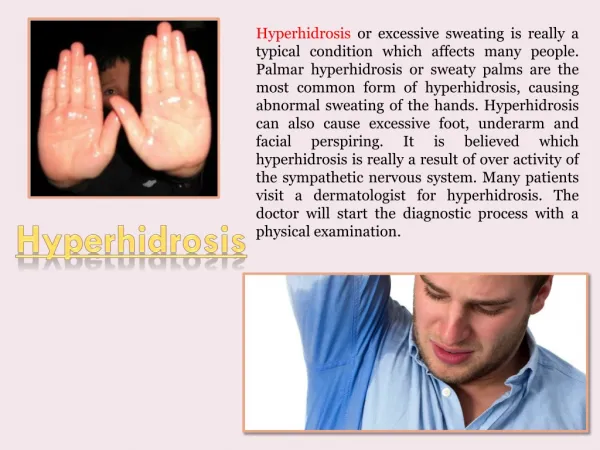
This clinical case discusses a 23-year-old female presenting with excessive palmar, axillary, and plantar perspiration. The patient has tried various treatments without relief. The case explores treatment options and the osteopathic approach to patient care.

E N D
SKIN DEEPA Clinical Case of Primary Hyperhidrosis Usaima Siddiqi Ahmad, PDTF, OMS IV Date of Patient Exam: Sep. 1, 2008 Student Year at That Time: OMS III Supervising Physician: Rebecca Giusti, D.O. COMP, Western University of Health Sciences
Case CC: “sweaty hands, armpits, and feet” HPI A 23 y/o female presents with excessive palmar, axillary, and plantar perspiration that began at age eleven, near the time of menarche. She states that warm to hot temperatures, stress (emotional or physical), and anxiety exacerbate her condition, while colder temperatures and a full night of sleep are palliative. Once started, symptoms tend to persist throughout the entire day without relief.
HPI Continued She has tried prescription strength deodorants, topical solutions, and iontophoresis without relief. She has a prescription for anti-cholinergics, but has not tried them due to feared side effects. Pt. states she is currently a 6/10 on a “Perspiration” scale that we developed together Perspiration Scale 0 = asymptomatic 5 = “clamminess” in affected areas 10= “dripping” sweat from affected areas No associated symptoms noted, per patient
PMH, SxH, Rxs, Allergies, FH PMH: unremarkable; no falls, trauma, motor vehicle accidents SxH: unremarkable Medications: none Allergies: NKDA, no environmental allergies FH: Healthy parents. Brother has palmar hyperhidrosis (much less severe, per pt).
Social History OMS-I Single, not sexually active No tobacco use, marijuana use, or other illicit drug use Occasional/social alcohol use Caffeine: One 12 oz. cup per day Psychosocial Stressors Boundaries Personal relationships: hand holding Professional life: hand shaking, stains on clothing
Physical VS, HEENT, CV, Resp, and Abd Exam Deferred Extremities Pulses intact bilaterally in UE and LE No clubbing, cyanosis, nor edema noted Neurological Gait: N CN II- XII grossly intact Sensation: Grossly intact over UE and LE B/L and trunk DTRs: +2/4 patellar and biceps, bilaterally
Structural Exam, At Initial Visit Head (H) Increased venous congestion, SBS compression, restricted right OM suture Cervical Region (C) OA: FRLSR, C3-6 FRRSR TART changes noted throughout region Thoracic Region (T) Restricted Supraclavicular fossa, B/L T2-3 NRLSR, T7-9 ERRSR
Initial Structural Exam, Cont Ribs (R) Right Rib 1: Inh SD, Left Rib 5: Inh SD Lumbar Region (L) L1-2 FRLSL, L5ERLSL Hypertonicity in paravertebral mm. B/L Sacral Region (S) R/L sacral torsion Upper Extremities (UE) Tenderness during passive ROM of right glenohumeral joint
Assessment 1. SD of the H,C, T, R, L, S, UE 2. Primary Focal Hyperhidrosis Isolated to the following areas: Axillary Palmar Plantar As opposed to Secondary or Generalized Hyperhidrosis
Hyperhidrosis Unknown Etiology ? Genetic component FH is a component in ¼ of patients Primary vs. Secondary Adolescence vs. Any time in life Craniofacial, axillary, palmar, plantar, full body 0.6-1.0% of population is effected “Occasional” spontaneous regression after age 35 Palmar or plantar keratoderma may occur
Treatment Options and Side Effects Home Remedies- cornstarch Low efficacy for most patients OMM Tx Reaction, rarely permanent Deodorants (OTC and Prescription) Only effective for axillary type Skin irritation, low efficacy in moderate-severe cases Topical Agents (aluminum based) Skin irritation, low efficacy in moderate-severe cases Theoretically oncogenic Anticholinergics Blurry vision, dry mouth, dry membranes, urinary retention, constipation, anorexia Iontophoresis Expense, time consuming- daily, and may cause dermatitis Botulinum Toxin (BTX-A) Expense, painful, results last about 4 months Repetitive injections Endoscopic Transthoracic Sympathectomy (ETS) and Lumbar Sympathectomy Surgical procedure, Horner’s Syndrome, compensatory hyperhidrosis
Biomechanical Address Somatic Dysfunction Recurrent findings on patient OA and T2-3 somatic dysfunctions, sacral torsion
Regions Addressed Head: SBS Decompression Venous Sinus Drainage HVLA to OA Suboccipital Release Thoracics and Lumbars: HVLA, ME, ST, MFR Ribs: BLT, HVLA Pelvis and Sacrum: ME, CrS Cervicals: BLT, ST, MFR Neurofascial Release Also performed during Tx 3-4
Neurological Balancing the Autonomic Nervous System OMT to cervical and sacral areas for parasympathetic balance OMT to thoracic, lumbar, and costal regions for sympathetic balance
Autonomic Control Sympathetic: Parasympathetic: Vagus Nerve: exits cranium near OA Sympathetic Chain T1-L2 Sacral Plexus S2-S4
Circulatory/Respiratory and Metabolic “…Localized segmental insults to the musculoskeletal system… produced rather substantial disturbances in the sympathetic function, at least as reflected in sweat-gland activity and in vascular and circulatory changes.” –I.M. Korr OMT to transition zones improved C/R functions 1Relieving somatic dysfunction leads to: Decreased energy demand Decreased energy expenditure 1Buzzell, 1970
Biopsychosocial Online Support Groups www.thedailystrength.org, www.hyperhidrosis.org, facebook.com Classmates Decreased severity of condition with treatments Increased social contact Decreased anxiety in social situations
Outcomes *Data Obtained Sep 2008
Conclusion Students can make a difference This case illustrates that OMM can influence autonomic function Structure influences function at many different levels
References Buzzell, Keith A. “The Cost of Human Posture.” The Physiological Basis of Osteopathic Medicine. Pg63-72. New York: Post Graduate Institute of Osteopathic Medicine and Surgery,1970. Pg63-72. Kuchera, William A., and Michael L. Kuchera.”Research and the Osteopathic Concept.” Osteopathic Principles in Practice. 2nd ed. Kirksville, Mo.: Kirksville College of Osteopathic Medicine, 1991. Print. Kuchera and Kuchera. Korr, Irvin M. The Collected Papers of Irvin M. Korr. Ed. Barbara Peterson. Colorado Springs: American Academy of Osteopathy, 1979. Print. Korr, Irvin M. "The Segmental Nervous System as a Mediator and Organizer of Disease Processes." The Physiological Basis of Osteopathic Medicine. New York: Postgraduate Institute of Osteopathic Medicine and Surgery, 1970. Print. Pg 73-84. Fealey Robert D, Sato Kenzo, "Chapter 82. Disorders of the Eccrine Sweat Glands and Sweating.” Wolff K, Goldsmith LA, Katz SI, Gilchrest B, Paller AS, Leffell DJ: Fitzpatrick's Dermatology in General Medicine, 7e: http://www.accessmedicine.com/content.aspx?aID=2985825. Low Phillip A, Engstrom John W, "Chapter 370. Disorders of the Autonomic Nervous System." Fauci AS, Braunwald E, Kasper DL, Hauser SL, Longo DL, Jameson JL, Loscalzo J: Harrison's Principles of Internal Medicine, 17e: www.accessmedicine.com/content.aspx?aID=2906166. http://www.accessmedicine.com/content.aspx?aID=2906166. Ropper AH, Samuels MA, "Chapter 26. Disorders of the Autonomic Nervous System, Respiration, and Swallowing.” Ropper AH, Samuels MA: Adams and Victor's Principles of Neurology, 9e: http://www.accessmedicine.com/ content.aspx?aID=3634223.