Download
1 / 67
670 likes | 672 Views
This informative book explores the organization of skeletal muscle, including connective tissue compartments, histopathologic features of muscle diseases, and various staining techniques used in muscle biopsy analysis. It covers topics such as muscle spindles, neuromuscular junctions, sarcomere structure, and classification of myopathies.

E N D
Diseases of Muscle:Histopathologic Features David Lacomis, MD
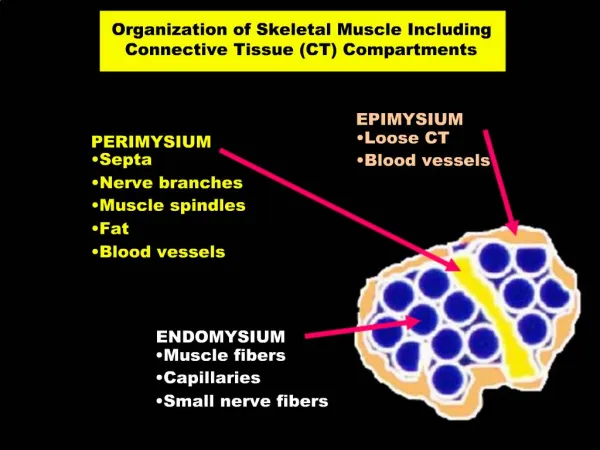
Organization of Skeletal Muscle Including Connective Tissue (CT) Compartments EPIMYSIUM PERIMYSIUM • Loose CT • Blood vessels • Septa • Nerve branches • Muscle spindles • Fat • Blood vessels ENDOMYSIUM • Muscle fibers • Capillaries • Small nerve fibers
Normal H&E-Stained Frozen Cross-Section of Skeletal Muscle Perimysial connective tissue Endomysial connective tissue • Note uniform sizes, polygonal shapes, and eccentric nuclei.
Normal H&E-Stained Longitudinal Paraffin Section • Note the banding pattern. • Nuclei are eccentrically placed.
Normal Structures: Muscle Spindle and Associated Nerve Fibers (Gomori trichrome) Spindle Nerve Twig
Neuromuscular Junctions • Can be identified by the esterase reaction due to the presence of acetylcholinesterase.
Neuromuscular Junction (Electron Microscopy) presynaptic postsynaptic
Histochemical Staining Intensity Based on Fiber Types NADH= nicotinamide adenine dinucleotide SDH= succinic dehydrogenase ATPase= adenosine triphosphatase
Normal (ATPase pH 9.4) • Type I fibers are light • Type II fibers are dark (pattern reverses at ATPase pH 4.3)
*Extends from Z-band to Z-band. A band includes overlap of actin and myosin. Note arrangement of thick and thin filaments. Ultrastructure of a Sarcomere* Actin Myosin I band I band H band M Z Z A band
Normal (Electron Microscopy) • Dark A-bands • Light I-bands • Z-band is present in the middle of the light band • Thin filaments are attached at the Z-band
Muscle Biopsy • Often necessary for final diagnosis of myopathy • Choose site based on clinical, electrodiagnostic, or imaging features • Avoid “end-stage” fatty muscle • Frozen sections most useful • Routine stains • Histochemistry • Immunohistochemistry
In all myopathies, degenerating fibers stain pale initially and then become digested by macrophages. Mononuclear inflammatory cell infiltrates and many basophilic regenerating fibers (arrow) Polymyositis(Longitudinal Paraffin-Embedded Section)
Regenerating fiber (non-specific) Fiber is basophilic due to presence of increased RNA and DNA. Activated plump nuclei and prominent nucleoli Polymyositis(Longitudinal Paraffin-Embedded Section-Higher Power)
Polymyositis(Longitudinal Paraffin-Embedded Section-Higher Power) • As regeneration advances, a myotube “bridge” is formed.
Invasion of a Non-necrotic Fiber by Inflammatory Cells • Seen in polymyositis, inclusion body myositis, and a few dystrophies.
Myophagocytosis(Esterase Stain) • Macrophages are ingesting the remnants of a degenerating fiber. This is a non-specific myopathic finding.
Dermatomyositis • Perifascicular atrophy & Degeneration • Perimysial nflammatory cells surround a blood vessel. • Inflammatory cells tend to be B-cells. • Vasculitis with bowel infarction and subcutaneous calcifications sometimes occur in the childhood form.
MAC is the terminal component of the complement pathway. It is often deposited in capillaries in dermatomyositis. Membrane Attack Complex (MAC)(Immunohistochemical Stain)
Inclusion Body Myositis (IBM) Invaded fiber • Features of chronic myopathy with endomysial inflammation and rimmed vacuoles are characteristic. Vacuole
Lymphocytic inflammation “Rimmed vacuoles”
(Congo Red) • IBM: Vacuoles contain amyloid.
IBM Intracytoplasmic (within Vacuoles) or Intranuclear Filamentous Inclusions
Granulomatous Myositisin a Patient with Sarcoidosis Giant cell • Granulomas tend not to cause significant damage to adjacent myofibers.
Endocrine Disturbance Type II Fiber Atrophy(ATPase pH9.4) • Characteristic of most endocrine myopathies and steroid myopathy
Inherited PolyneuropathyChronic Neurogenic Atrophy • Groups of angulated atrophic fibers • Marked variation in myofiber size
Acute Denervation(NADH Reaction) • Manifested by small, darkly staining angulated fibers.
Denervation(Esterase Stain) • Denervated fibers also stain darkly with non-specific esterase.
Chronic Neurogenic Processes(NADH Reaction) • Target fibers noted. • Light center surrounded by a darker rim. • Generally only seen in type I fibers.
Chronic Neurogenic Atrophy(ATPase Reaction) • Fiber type grouping
Opaque or hyaline fibers (arrows) Increase in endomysial connective tissue Frozen Section from a Patient withDuchenne Muscular Dystrophy Group of basophilic regenerating fibers
Normal Immunohistochemical Stain for Dystrophin(Subsarcolemmal Staining)
Duchenne Muscular Dystrophy (Absent Staining for Dystrophin)
Becker Muscular Dystrophy (Reduced but Present Staining) split fiber (non-specific chronic change)
Female Carrier of Duchenne Muscular Dystrophy (A Mosaic Staining Pattern)
Locations of Affected Proteinsin Muscular Dystrophies Extracellular Matrix Laminin-2 Dystroglycan complex a g b a b sarcoglycans Sarcolemma Lamin A/C (emerin) Caveolin 3 Dysferlin Dystrophin nucleus Actin
Emery-Dreifuss Muscular Dystrophy(Gomori Trichrome-Stained Frozen Section) Necrotic fiber • Variation in fiber size with many hypertrophic fibers • Increase in endomysial connective tissue • Nonspecific so-called dystrophic changes seen in many of the muscular dystrophies. • Can also be seen in any chronic myopathic disorder. • This disorder is due to loss of the protein emerin.
Myotonic Dystrophy • Chronic changes • Marked excess in internalized nuclei • Variation in fiber sizes • Nuclear clumps (not shown)
(H & E, Paraffin) • The excess of internalized nuclei can lead to nuclear chains.
Myotonic Dystrophy(NADH-Reacted Section) • Ring fibers in which myofilaments are organized in different directions
The majority of dystrophies do not have a specific histopathologic appearance. Clinical features are also very important. For example, winging of the scapula is characteristic of FSHD. Fascioscapulohumeral Dystrophy (FSHD)
Variable non-specific changes Range from scattered atrophy to “dystrophic” features. Inflammation can be present (arrow). FSH Dystrophy
Central areas of absent staining in the dark type I fibers Mitochondria absent Congenital Myopathies: Central Core Myopathy(NADH)
Congenital Myopathies: Central Core Myopathy(NADH) • The core consists of disorganized myofibrils and the area is devoid of mitochondria.
Congenital Fiber Type Disproportion(H&E) • Bimodal size population
Congenital Fiber Type Disproportion(ATPase pH 4.3) • Smaller fibers are type I • More numerous • Stain lightly • Larger or normal fibers are type II
Nemaline Myopathy • Eosinophilic inclusions present.