Download
1 / 50
500 likes | 502 Views
This presentation discusses the FDA-approved indication of nebivolol, its appropriate initial dosage and titration schedule, potential drug interactions, mechanism of action, and unique advantages compared to other medications in its class for the treatment of hypertension.

E N D
for treatment of hypertension Novel Therapy or another “me too” drug? Mark Pellegrini, PharmD
Nebivolol: Objectives • Upon successful completion of the presentation, the attendees will be able to: • Identify the FDA approved indication of nebivolol, as well as the appropriate initial dosage of nebivolol to treat hypertension, and the correct titration schedule. • Identify potential drug interactions for nebivolol. • Explain the mechanism(s) of action for nebivolol. • Summarize any unique advantages of nebivolol compared to other medications in its class.
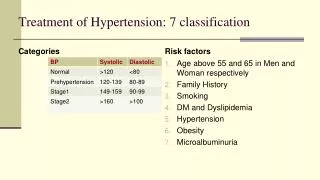
Hypertension & Therapy Goals • HTN - the numbers: • Affects approximately 50 million Americans • One billion affected world-wide • Fewer than 60% affected receive any treatment • Only 31% have adequate control • JNC-7 Goals: • Chobanian AV, Baksris GL, Black HR, et al.. JAMA 2003;289:2560–2572. • Hajjar I, Kotchen TA. 0. JAMA 2003:290:199–206.
1° Hypertension: Pathogenesis Potential mechanisms of Pathogenesis: 1.) Increased Cardiac Output: • Increased cardiac preload: • ↑ fluid volume from excess Na intake or renal • Na retention (↓ GFR or # of nephrons) • Venous Constriction: • Excess RAAS stimulation • Excess sympathetic NS stimulation 2.) Increased PVR: • Functional Vascular Constriction/Hypertrophy: • Excess RAAS stimulation • Sympathetic NS overactivity • Endothelial-derived factors • Genetic alterations of cell membranes • Hyperinsulinemia from obesity or metabolic syndrome Joseph T. DiPiro, et al, ed; Pharmacotherapy – A Pathophysiologic Approach,
Beta Blockers: MOA • Cardiac Effects – β blockade • Negative inotropy - ↓ contractility • Negative lusitropy - ↓ relaxation rate • Negative chronotropy - ↓ heart rate • Negative dromotropy - ↓ conduction rate Image: http://www.cvpharmacology.com/cardioinhibitory/beta-blockers.htm
Beta Blockers: MOA Vascular Effects β2 blockade α blockade (3G) Smooth muscle contraction - (mild vasoconstriction) Smooth muscle relaxation (mild vasodilatation) Man in’t Veld, AJ, et al. Am J Hypertens. 1988;1:91-96 Images: http://www.cvpharmacology.com/cardioinhibitory/beta-blockers.htm http://www.cvpharmacology.com/vasodilator/alpha.htm
Beta-Blockers: By the Numbers • LexiComp Online
Nebivolol: General Information • Nebivolol is a 3rd Generation β-adrenergic blocker • In extensive metabolizers (most of the population) it is preferentially β1selective at doses of < 10 mg. • In poor metabolizers & at higher doses it does exhibit both β1 &β2-adrenergic inhibitory activity. • Said to have Nitric Oxide mediated vasodilatory effects & anti-oxidant properties • Has been approved in Europe for mild/moderate HTN & HF, FDA approved for HTN; October of 2007 • Weiss, Robert, Vasc Health Risk Manag. 2006 September; 2(3): 303–308 • BYSTOLIC [package insert]. St. Louis, MO: Forest Pharmaceuticals, Inc.; 2008. • de Boer, Voors, van Veldhuisen, Expert Opinion on Pharmacotherapy, July 2007
Nebivolol: General Information • Nebivolol is a racemate of both d & l-nebivolol; • chemical formula = C22H25F2NO4•HCl BYSTOLIC [package insert]. St. Louis, MO: Forest Pharmaceuticals, Inc.; 2008.
Nebivolol: General Information • Available in 2.5, 5, 10, & 20 mg tablets. Pictures: online.epocrates.com
Nebivolol: Recommended Dosing • Individualized to patient needs • Recommended starting dose is 5 mg daily • Can be used as monotherapy or in conjunction with other hypertensive agents • If further BP reduction needed, can be increased in 2 week intervals • Maximum daily dose 40 mg daily • May be administered without regard to meals BYSTOLIC [package insert]. St. Louis, MO: Forest Pharmaceuticals, Inc.; 2008.
Nebivolol: Side Effects Profile Baldwin and Keam, Am J Cardiovasc Drugs 2009; 9 (4): 253-260
Nebivolol: Pharmacodynamics • “MOA of hypertensive response has not been definitively established.” Possible factors include: • Decreased heart rate • Decreased contractility of myocardium • Reduction of sympathetic mediated tonicity by cerebral vasomotor centers • Renin suppression • Reduced PVR and vasodilation BYSTOLIC [package insert]. St. Louis, MO: Forest Pharmaceuticals, Inc.; 2008.
Nebivolol: Contraindications • Severe bradycardia • Greater than 1st degree heart block • Cardiogenic shock • Decompensated heart failure • Sick sinus syndrome (without pacemaker) • Sever hepatic impairment (Child-Pugh > B) • Hypersensitivities to product or components • Pregnancy category: C • Lexicomp Online; Bystolic; www.crlonline.com • Baldwin and Keam, Am J Cardiovasc Drugs 2009; 9 (4): 253-260
Nebivolol: Pharmacokinetics • Active d-isomer has 1,000 times greater affinity for beta-receptors than does the l-isomer • For same dose, PMs obtain about a 5X greater Cmax & 10-fold higher AUC for d-nebivolol than do EMs • Mean peak plasma concentrations occur between 1.5 to 4 hours after administration (EM and PM) • In vitro human PPB is 98%; mostly albumin; concentration independent • Adjust dose in renal impairment (CrCl < 30 mL/min) Baldwin and Keam, Am J Cardiovasc Drugs 2009; 9 (4): 253-260
Nebivolol: Metabolism & Excretion • Predominantly metabolized via glucuronidation of parent drug • Also to a lesser extent by N-dealkylation and oxidation via CYP2D6. • Tests on single oral administration of radio-isotoped nebivolol revealed: • EMs: 38% recovered in urine & 44% in feces • PMs: 67% recovered in urine & 13% in feces BYSTOLIC [package insert]. St. Louis, MO: Forest Pharmaceuticals, Inc.; 2008.
Nebivolol: Metabolism & Interactions • Inhibitors and inducers of CYP2D6 can affect plasma concentration levels. • When administered with CYP2D6 inhibitors or inducers, patient should be closely monitored, and dosages adjusted according to hypertensive response • In vitro studies revealed that neither isomer of nebivolol inhibited any CYP450 pathways at therapeutically relevant concentrations BYSTOLIC [package insert]. St. Louis, MO: Forest Pharmaceuticals, Inc.; 2008.
Nebivolol: Metabolism & Interactions Pharm Letter 2006;1–5.
Nebivolol: Metabolism & Interactions • Other interaction “pearls”: • Nebivolol should be avoided in patients taking other myocardial depressants: e.g. DHP CCBs, or antiarrythmia agents • ↑ risk of bradycardia • Digoxin & warfarin studied in small trials • No alteration of pharmacokinteics of any agents • Small study showed that ramipril and furosemide also had no pharmacokinetic interactions • ACE-I & diuretics often used in HTN combination therapy
Nebivolol & Oxidative Stress • In vivo treatment with nebivolol markedly improved endothelial dysfunction and NO signaling in vessels from hypercholesterolemic rabbits…secondary to normalization of superoxide production. • Other β-blockers, such as atenolol and metoprolol, were not able to inhibit superoxide production. • May explain why nebivolol but not metoprolol is able to reduce the progression of atherosclerosis in the setting of hypercholesterolemia. Oelze, Daiber, Brandes, et al, Hypertension 2006;48;677-684
Nebivolol & Arterial Stiffness • Arterial distensibility, measured by pulse wave velocity (PWV); study performed on sheep, comparing effects of nebivolol to atenolol • Study concluded: • “…nebivolol, but not atenolol, causes peripheral vasodilatation via the release of NO.” • “…endothelium-derived NO, to a large extent, mediates the effect of nebivolol on PWV…at clinical doses, nebivolol increases stimulated and basal production of NO in patients with essential hypertension.” Avolio, Wilkinson, Cockroft, et. al, Hypertension 2004;44;305-310
Nebivolol: NO & Vasodilation • A series of small studies on rodents and a small sample of humans concluded: • “Nebivolol dilates human and rodent coronary resistance microarteries through an agonist effect on endothelial β3-adrenoreceptors to release NO and promote neoangiogenesis.” • “These properties may prove particularly beneficial for the treatment of ischemic and cardiac failure diseases through preservation of coronary reserve.” Dessy, Saliez, Ghisdal, et. al; Circulation. 2005;112:1198-1205
Nebivolol: FDA Warning Letter • Ad suggested that Bystolic is “safer and more effective than has been demonstrated by substantial evidence.” • "...a novel beta blocker" (page 1); • "Next generation beta blocker" (pages 1, 3, 5, 7); and • "Unique mechanism of action includes cardioselective beta blockade and vasodilation" (pages, 3,4). • "Favorable tolerability profile with a low incidence of beta blocker related side effects" (page 3); and • "... favorable tolerability profile" (pages 2, 7). • The FDA: “The above claims misleadingly imply that the tolerability profile of Bystolic is better than…other ß-adrenergic receptor blocking agents…has not been demonstrated by substantial evidence or substantial clinical experience. “ • “The journal ad makes unsubstantiated superiority and mechanism of action claims…and makes unsubstantiated efficacy claims for the drug.” • “Thus, the journal ad misbrands the drug in violation of the Federal Food, Drug, and Cosmetic Act…” • August, 2008 letter to Forest Laboratories, Inc. • Review of an 8-Page Launch Journal Ad
Pivotal Study 1: Design • “A Randomized, Double-Blind, Placebo-Controlled Parallel-Group Study to Assess the Efficaacy and Safety of Nebivolol, a Novel β-Blocker, in Patients With Mild to Moderate Hypertension” • Phase III, 12 weeks duration at 70 sites • 4 week, single-blind, placebo run-in/wash-out period • Post screening and before randomization • Patients previously on HTN meds; additional 2 weeks • 909 patients, 777 completed study (85%) • US Code of Federal Regulations, Good Practice Guidelines Weiss, et al. J Clin Hypertens. 2007;9(9):667-676
Pivotal Study 1: Criteria • Inclusion Criteria • Males & females 18 and older • Mild to moderate HTN (SiDBP ≥ 95 & ≤109) • Exclusion Criteria • Secondary or malignant HTN • BMI > 35, uncontrolled DM, recent MI/stroke, HF • Clinically significant thyroid, renal, hepatic dysfunction • Bronchospasm, bradycardia, or other known contraindication to β-blocker, prior nebivolol use • 9.7% DM, 43.9% obese (BMI > 30) Weiss, et al. J Clin Hypertens. 2007;9(9):667-676
Pivotal Study 1: Endpoints • Primary Endpoints: • Change in trough SiDBP from baseline to day 84 • (24 +/- 2 hours from previous morning dose) • Secondary Endpoints: • Change in trough SiSBP from baseline to day 84 • Mean SiDBP & SiSBP at peak • (2-3 hours post dose) • Mean supine & standing trough & peak SiSBP/SiDBP • Responder rate at day 84: • Proportion of pts with SiDBP < 90 or ≥10 reduction Weiss, et al. J Clin Hypertens. 2007;9(9):667-676
Pivotal Study 1: Results • 909 randomized • 777 completed study (85.5%) • 82.7% placebo; 85.7% treatment • Most common reasons for discontinuance: • Withdrawn consent (5.3%) • AEs (2.5%) • Loss to follow-up (2.5%) • 12 serious AEs; 11 treatment, 1 placebo • Only 2 in treatment group were considered drug related (ECG changes – resolved spontaneously)
Pivotal Study 1: Results Placebo-subtracted least squares mean reductions Green; P < .001 Yellow; P = .002 n: Placebo = 81 1.25 = 83 2.5 = 81 5 = 165 10 = 166 20 = 166 40 = 166 Weiss, et al. J Clin Hypertens. 2007;9(9):667-676
Study 1: Strengths/Weaknesses • Strengths • Double blind • Placebo controlled • Multi center • Intent to treat • Good demographic stratification • Weaknesses • One of the authors works for Forest Pharmaceuticals • Only 14.5% African-American patients
Pivotal Study 1: Conclusion • “Nebivolol…is an effective antihypertensive agent in patients with mild to moderate hypertension. It is well tolerated, with a low incidence of AEs such as fatigue, depression, and ED that are associated with other β-blockers.” Weiss, et al. J Clin Hypertens. 2007;9(9):667-676
Pivotal Study 2: Design • “The Efficacy and Tolerability of Nebivolol in Hypertensive African American Patients” • Phase III, 12 week, 39 site, double blind, placebo controlled study • 301 patients randomized (45% male) • 28 day, single blind run-in period • Additional 14 days for patients previously on antihypertensive agents • Stratified across groups by metabolizer status, DM, age (>/< 65), and gender Saunders, et al, J Clin Hypertens. 2007;9(11):866-875
Pivotal Study 2: Criteria • Inclusion Criteria: • African American males & females • 18 years and older • Stage I or II HTN (SiDBP ≥ 95 and ≤ 109) • Exclusion Criteria • Secondary or malignant HTN • BMI > 40 or uncontrolled Type II DM (A1C ≥ 10) • COPD • MI/Stroke within 6 months of study • Significant renal or hepatic disease • Sensitivity to β-blockers • Pregnant, breast feeding, or child-bearing years & no contraception Saunders, et al, J Clin Hypertens. 2007;9(11):866-875
Pivotal Study 2: Endpoints • Primary Endpoints: • Change in trough SiDBP from baseline to day 84 • (24 +/- 2 hours from previous morning dose) • Secondary Endpoints: • Change in trough SiSBP from baseline to day 84 • Mean SiDBP & SiSBP at peak • (2-3 hours post dose) • Mean supine & standing trough & peak SiSBP/SiDBP • Responder rate at day 84: • Proportion of pts with SiDBP < 90 or ≥10 reduction Saunders, et al, J Clin Hypertens. 2007;9(11):866-875
Pivotal Study 2: Results • 568 screened • 485 entered the single blind placebo phase • 300 randomized • 259 completed study (86.3%) • 83.7% placebo; 86.8% treatment • Most common reasons for discontinuance: • Treatment failure (3.3%) • Loss to follow-up (3.0%) • AEs (2.0%) Saunders, et al, J Clin Hypertens. 2007;9(11):866-875
Pivotal Study 2: Results Placebo-subtracted least squares mean reductions n: Placebo = 49 2.5 = 49 5 = 50 10 = 51 20 = 50 40 = 51 Orange = not significant to placebo Yellow: P = .004 Green: P ≤ .001 Blue: P ≤.045 Saunders, et al, J Clin Hypertens. 2007;9(11):866-875
Pivotal Study 2: Results Response Rates by Treatment at day 84 (SiDBP < 90 or ≥10 reduction) Orange = not significant to placebo Yellow: P = .002 Green: P ≤ .001 Saunders, et al, J Clin Hypertens. 2007;9(11):866-875
Study 2: Strengths/Weaknesses • Strengths • Double blind, placebo controlled, multi center • Intent to treat • No age limit • Weaknesses • One author sponsored by Forest Pharmaceuticals • Smaller study population (n = 301) • Low percentage of diabetic patients (14.3%) • No baseline renin levels were taken Saunders, et al, J Clin Hypertens. 2007;9(11):866-875
Pivotal Study 2: Conclusion • “Nebivolol monotherapy is safe and effective in lowering BP in hypertensive African American patients. While nebivolol has hemodynamic actions that may be favorable in this population, further studies are needed to determine whether these specific actions contribute significantly…to clinical outcomes.” Saunders, et al, J Clin Hypertens. 2007;9(11):866-875
Pivotal Study 3: Design • “Adding nebivolol to ongoing antihypertensive therapy improves blood pressure and response rates in patients with uncontrolled stage I-II hypertension” • Phase III, 12 week, randomized, double-blind, placebo-controlled parallel group study at 96 centers • Patients taking β-blocker underwent a 14 day wash-out • Assessments at days 14, 42, & 84 • Concomitant therapy with CCB, opthalmic β-blockers, α1-receptor blockers, & long-acting oral nitrates prohibited for duration of study Neutel, et al, Journal of Human Hypertension, 30 April 2009; doi: 10.1038/jhh.2009.33
Pivotal Study 3: Criteria • Inclusion Criteria • Males & females 18 and older, currently treated for stage I-II HTN with up to2 of the following; ACE-I, ARB, or diuretic • Mild to moderate inadequately controlled HTN (SiDBP ≥ 95 & ≤109) • Exclusion Criteria • Secondary or malignant HTN • BMI > 35, uncontrolled type II DM (A1C ≥ 10) • Recent MI/stroke, HF requiring treatment • Severe PVD, significant valvular heart disease • Clinically significant thyroid, renal, hepatic dysfunction • Respiratory disorders, bradycardia (< 50 BPM), or other known contraindication to β-blocker, use of CCB Neutel, et al, Journal of Human Hypertension, 30 April 2009; doi: 10.1038/jhh.2009.33
Pivotal Study 3: Endpoints • Primary Endpoints: • Change in trough SiDBP from baseline to day 84 • (24 +/- 3 hours from previous morning dose) • Secondary Endpoints: • Change in trough SiSBP from baseline to day 84 • Mean SiDBP & SiSBP at peak • (2-3 hours post dose) • Mean supine & standing trough & peak SiSBP/SiDBP • Responder rate at day 84: • Proportion of pts with SiDBP < 90 or ≥10 reduction Neutel, et al, Journal of Human Hypertension, 30 April 2009; doi: 10.1038/jhh.2009.33
Pivotal Study 3: Results • 1171 screened, 669 randomized • 55% male, mean age was 53 years • 55% Caucasian, 29% AA, 15% Hispanic, 1% Asian • 14.1% diabetic • 598 completed study (89.4%) • Placebo 87.45%, treatment 90.0% • Most common reasons for discontinuance: • Withdrawn consent (4.0%) • AEs (3.7%) • Lost to follow-up (1.5%) Neutel, et al, Journal of Human Hypertension, 30 April 2009; doi: 10.1038/jhh.2009.33
Pivotal Study 3: Results Placebo-subtracted least squares mean reductions n: Placebo = 167 5 = 168 10 = 168 20 = 166 Orange = not significant to placebo Yellow: P < .001 Green: P = .015 Neutel, et al, Journal of Human Hypertension, 30 April 2009; doi: 10.1038/jhh.2009.33
Pivotal Study 3: Results Response Rates by Treatment at day 84 (SiDBP < 90 or ≥10 reduction) n: Placebo = 167 5 = 168 10 = 168 20 = 166 Orange = not significant to placebo Yellow: P < .001 Blue: P = .028 Violet: P = .001 Neutel, et al, Journal of Human Hypertension, 30 April 2009; doi: 10.1038/jhh.2009.33
Study 3: Strengths/Weaknesses • Strengths • Double blind, placebo controlled, multi center • Intent to treat • No age limit • High completion rate (89.4%) • Weaknesses • One author sponsored by Forest Pharmaceuticals • Didn’t differentiate between different existing HTN treatment regimens • The study title has bias/gives the results Neutel, et al, Journal of Human Hypertension, 30 April 2009; doi: 10.1038/jhh.2009.33
Pivotal Study 3: Conclusion • “Nebivolol as an add-on treatment was well tolerated…AEs being comparable to placebo at all doses.” • “Add-on therapy with nebivolol is an effective and well tolerated treatment option for patients with uncontrolled HTN, despite receiving background antihypertensive therapy.” Neutel, et al, Journal of Human Hypertension, 30 April 2009; doi: 10.1038/jhh.2009.33
Nebivolol: Conclusions • Nebivolol is a well-tolerated β-blocking agent that has been shown to successfully lower SiDBP in well designed studies on a variety of HTN patients • Useful in both mono & combined regimens • More US-based research needs to be performed on human subjects to determine if the NO2 mediated vasodilatory effects warrant “special status” among β-blocking agents • Many more studies on nebivolol have been conducted in Europe.
References-1 • Chobanian AV, Baksris GL, Black HR, et al. Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 7). JAMA 2003;289:2560–2572. • Hajjar I, Kotchen TA. Trends in prevalence, awareness, treatment, and control of hypertension in the United States,1988–2000. JAMA 2003:290:199–206. • BYSTOLIC [package insert]. St. Louis, MO: Forest Pharmaceuticals, Inc.; 2008 • Rudolf A de Boer, Adriaan A Voors, Dirk J van Veldhuisen, Nebivolol: third-generation β-blockade, Expert Opinion on Pharmacotherapy, July 2007, Vol. 8, No. 10 : pp. 1539-1550 • Weiss, Robert, Nebivolol: A Novel Beta-Blocker with Nitric Oxide-Induced Vasodilatation, Vasc Health Risk Manag. 2006 September; 2(3): pp. 303–308 • https://online.epocrates.com/ (Accessed 12/30/2009) • Lexicomp Online; Bystolic; www.crlonline.com (Accessed 1/2/2010) • Avolio, Ian B. Wilkinson and John R. Cockcroft, Carmel M. McEniery, Matthias Schmitt, Ahmad Qasem, David J. Webb, Alberto P., Nebivolol Increases Arterial Distensibility In Vivo, Hypertension 2004;44;305-310 • Matthias Oelze, Andreas Daiber, Ralf P. Brandes, Marcus Hortmann, Philip Wenzel, Ulrich Hink, Eberhard Schulz, Hanke Mollnau, Alexandra von Sandersleben, Andrei L. Kleschyov, Alexander Mülsch, Huige Li, Ulrich Förstermann and Thomas Münzel, Nebivolol Inhibits Superoxide Formation by NADPH Oxidase and Endothelial Dysfunction in Angiotensin II–Treated Rats; Hypertension 2006;48;677-684 • Chantal Dessy, PhD; Julie Saliez, BSc; Philippe Ghisdal, PhD; Géraldine Daneau, BSc; Irina I. Lobysheva, PhD; Françoise Frérart, BSc; Catharina Belge, MD; Karima Jnaoui, PhD; Philippe Noirhomme, MD; Olivier Feron, PhD; Jean-Luc Balligand, MD, PhD; Endothelial 3-Adrenoreceptors Mediate Nitric Oxide–Dependent Vasorelaxation of Coronary Microvessels in Response to the Third-Generation -Blocker Nebivolol, Circulation. 2005;112:1198-1205
References-2 • Thomas Abrams, FDA Warning Letter, August 28, 2008, retrieved from www.fda.gov (Accessed 1/1/2009) • Heather Won Tesoriero, ‘Hey, Nineteen,’ We Say to Beta Blocker Come-Lately, Wall Street Journal Online, 12/18/2007, (Accessed 1/1/2009) • Claudine M. Baldwin and Susan J. Keam, Nebivolol In the Treatment of Hypertension in the US, Am J Cardiovasc Drugs 2009; 9 (4): 253-260 • Robert J. Weiss, MD, Michael A. Weber, MD, Albert A. Carr, MD, Will A. Sullican, BS; A Randomized, Double-Blind, Placebo Controlled Parallel Study Group Study to Assess the Efficacy and Safety of Nebivolol, A Novel B-Blocker, in Patients With Mild to Moderate Hypertension, J Clin Hypertens. 2007;9(9):667-676 • Elijah Saunders, MD, William B. Smith, MD, Karen B. DeSalvo, MD, Will A. Sullivan, BS, The Efficacy and Tolerability of Nebivolol in Hypertensive African American Patients, J Clin Hypertens. 2007;9(11):866-875 • JM Neutel, DHG Smith and AH Gradman, Adding nebivolol to ongoing hypertensive therapy improves blood pressure and response rates in patients with uncontrolled stage I-II hypertension, Journal of Human Hypertension, 30 April 2009; doi: 10.1038/jhh.2009.33 • Richard E Klabund, PhD; http://www.cvpharmacology.com/cardioinhibitory/beta-blockers.htm (images), (Accessed 1/22/2010) • Cytochrome P450 drug interactions. Pharm Letter 2006;1–5. • Man in’t Veld AJ, Van den Mieracker AH, Schalekamp MA. Do beta-blockers really increase peripheral vascular resistance? Review of the literature and new observations under basal conditions. Am J Hypertens. 1988;1:91-96 • Joseph T. DiPiro, et al, ed; Pharmacotherapy – A Pathophysiologic Approach, 6th Edition, New York, McGraw-Hill, 2005, p. 187.