Download
1 / 1
10 likes | 151 Views
Management of Postherpetic Neuralgia with Intrathecal Methylprednisolone Vinaya K. Puppala , MD, Jessen Mukalel , MD, N. Nick Knezevic , MD, PhD, Kenneth D. Candido , MD Department of Anesthesiology, Advocate Illinois Masonic Medical Center, Chicago, IL 60657 USA. Abstract.

E N D
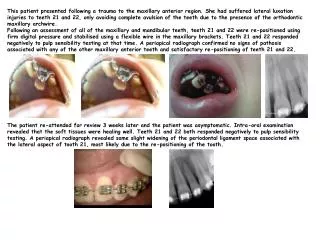
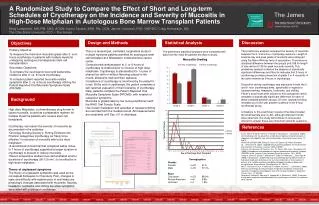
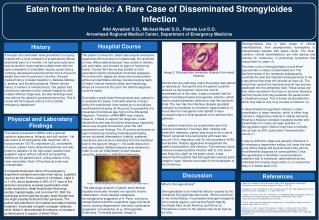
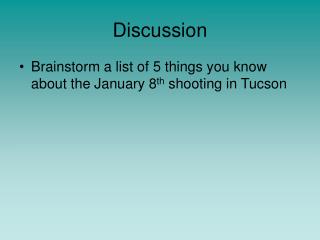
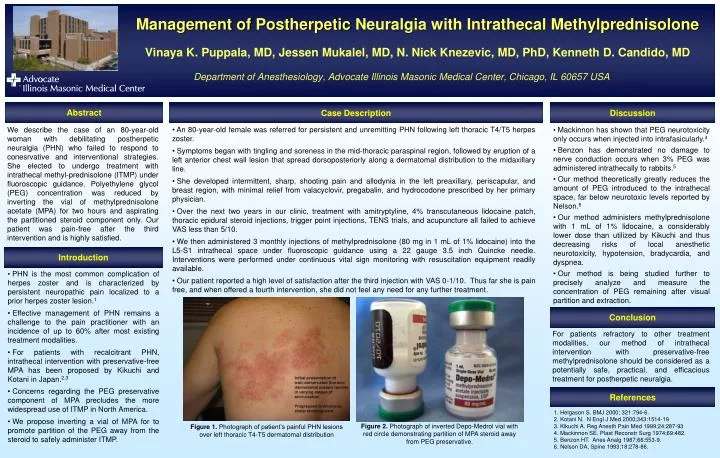
Management of Postherpetic Neuralgia with Intrathecal MethylprednisoloneVinaya K. Puppala, MD, JessenMukalel, MD, N. Nick Knezevic, MD, PhD, Kenneth D. Candido, MDDepartment of Anesthesiology, Advocate Illinois Masonic Medical Center, Chicago, IL 60657 USA Abstract Case Description Discussion • An 80-year-old female was referred for persistent and unremitting PHN following left thoracic T4/T5 herpes zoster. • Symptoms began with tingling and soreness in the mid-thoracic paraspinal region, followed by eruption of a left anterior chest wall lesion that spread dorsoposteriorly along a dermatomal distribution to the midaxillary line. • She developed intermittent, sharp, shooting pain and allodynia in the left preaxillary, periscapular, and breast region, with minimal relief from valacyclovir, pregabalin, and hydrocodone prescribed by her primary physician. • Over the next two years in our clinic, treatment with amitryptyline, 4% transcutaneous lidocaine patch, thoracic epidural steroid injections, trigger point injections, TENS trials, and acupuncture all failed to achieve VAS less than 5/10. • We then administered 3 monthly injections of methylprednisolone (80 mg in 1 mL of 1% lidocaine) into the L5-S1 intrathecal space under fluoroscopic guidance using a 22 gauge 3.5 inch Quincke needle. Interventions were performed under continuous vital sign monitoring with resuscitation equipment readily available. • Our patient reported a high level of satisfaction after the third injection with VAS 0-1/10. Thus far she is pain free, and when offered a fourth intervention, she did not feel any need for any further treatment. • Mackinnon has shown that PEG neurotoxicity only occurs when injected into intrafasicularly.4 • Benzon has demonstrated no damage to nerve conduction occurs when 3% PEG was administered intrathecally to rabbits.5 • Our method theoretically greatly reduces the amount of PEG introduced to the intrathecal space, far below neurotoxic levels reported by Nelson.6 • Our method administers methylprednisolone with 1 mL of 1% lidocaine, a considerably lower dose than utilized by Kikuchi and thus decreasing risks of local anesthetic neurotoxicity, hypotension, bradycardia, and dyspnea. • Our method is being studied further to precisely analyze and measure the concentration of PEG remaining after visual partition and extraction. We describe the case of an 80-year-old woman with debilitating postherpetic neuralgia (PHN) who failed to respond to conesrvative and interventional strategies. She elected to undergo treatment with intrathecal methyl-prednisolone (ITMP) under fluoroscopic guidance. Polyethylene glycol (PEG) concentration was reduced by inverting the vial of methylprednisolone acetate (MPA) for two hours and aspirating the partitioned steroid component only. Our patient was pain-free after the third intervention and is highly satisfied. Introduction • PHN is the most common complication of herpes zoster and is characterized by persistent neuropathic pain localized to a prior herpes zoster lesion.1 • Effective management of PHN remains a challenge to the pain practitioner with an incidence of up to 60% after most existing treatment modalities. • For patients with recalcitrant PHN, intrathecal intervention with preservative-free MPA has been proposed by Kikuchi and Kotani in Japan.2,3 • Concerns regarding the PEG preservative component of MPA precludes the more widespread use of ITMP in North America. • We propose inverting a vial of MPA for to promote partition of the PEG away from the steroid to safely administer ITMP. Conclusion For patients refractory to other treatment modalities, our method of intrathecal intervention with preservative-free methylprednisolone should be considered as a potentially safe, practical, and efficacious treatment for postherpetic neuralgia. References 1. Helgason S. BMJ 2000; 321:794-6. 2. Kotani N. N Engl J Med 2000;343:1514-19 3. Kikuchi A. Reg Anesth Pain Med 1999;24:287-93 4. Mackinnon SE. Plast Reconstr Surg 1974;69:482. 5. Benzon HT. Anes Analg 1987;66:553-9. 6. Nelson DA, Spine 1993;18:278-86. Figure 2. Photograph of inverted Depo-Medrol vial with red circle demonstrating partition of MPA steroid away from PEG preservative. Figure 1. Photograph of patient’s painful PHN lesions over left thoracic T4-T5 dermatomal distribution