Download
1 / 20
200 likes | 208 Views
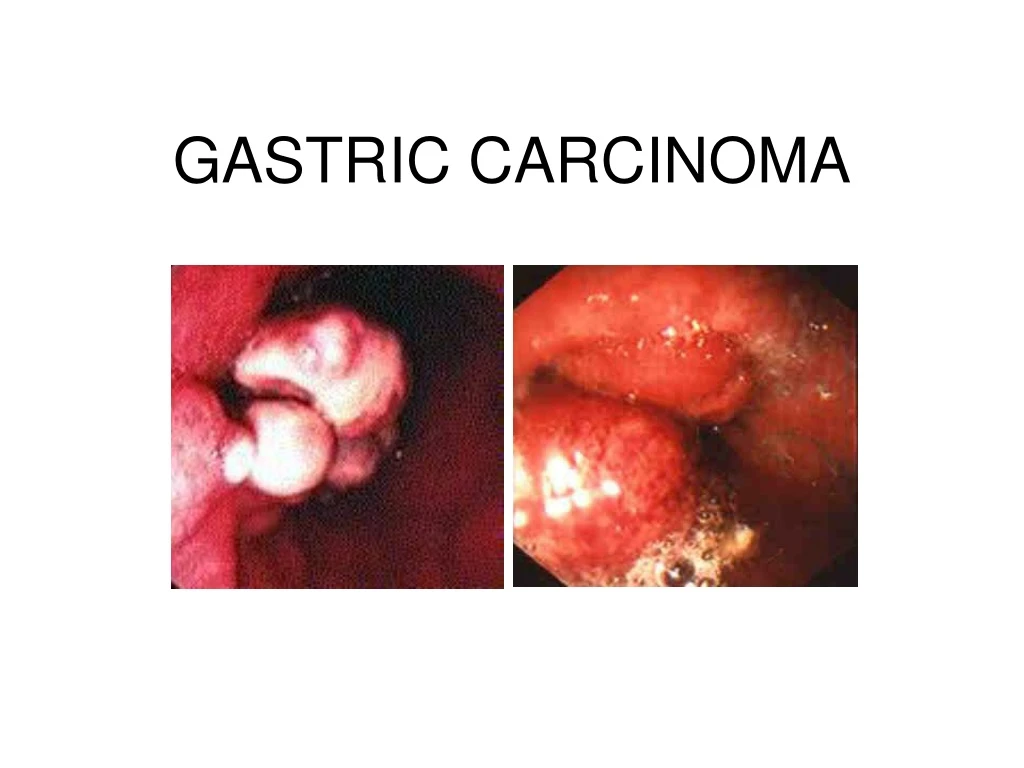
GASTRIC CARCINOMA. Pathophysiology. Adenocarcinoma characterized as intestinal or diffuse Spreads through stomach into the gastric wall to the Lymph nodes Liver Pancreas Transverse colon Omentum Peritoneum Ovaries Pelvic cul-de-sac Through portal vein into lungs, liver, and bone

E N D
Pathophysiology • Adenocarcinoma characterized as intestinal or diffuse • Spreads through stomach into the gastric wall to the • Lymph nodes • Liver • Pancreas • Transverse colon • Omentum • Peritoneum • Ovaries • Pelvic cul-de-sac • Through portal vein into lungs, liver, and bone • Advanced stage: stomach muscle
Etiology • H. pylori: 80 percent of gastric carcinomas result from H. pylori due to the result of free radicals • Dietary nitrates (bacteria in stomach breaks down nitrites to compounds that are carcinogenic in animals) • Hypochlorhydria: occurs in gastric atrophy and promotes bacterial growth in stomach • Foods such as starch, pickled vegetables, salted fish and meat, smoked foods and salt • People who smoke cigarettes or use alcohol are 3-5 times more likely
Etiology cont. • Epstein-Barr virus is now implicated as a cause • Pernicious anemia • Chronic atrophic gastritis • Gastric polyp • Achlorhydria • Barrett’s esophagus • Having had a Billroth 2 procedure • Genetic factors include: • First degree relatives • Type A blood
Incidence/Prevalence • 3rd most common GI malignancy (after colorectal and pancreatic) • 14th cause of cancer related death in U.S. • 85-95% are caused by adenocarcinoma • 15% are caused by Non-Hodgkin’s lymphoma & leiomysosarcomas
location • 37% in the proximal third of the stomach • 30% in the distal stomach • 20% in the midsection • Remaining 13% in the entire stomach
Onset • Insidious (slowly developing) • Usually discovered in advanced stages • Men>Women • Occurs between the ages of 50-70 • Increased mortality in • Japanese • Costa Ricans • Chileans • Native Americans • African Americans • Scandinavians
Assessment • History: • High risk foods • Alcohol/tobacco use • Treated for H. Pylori infection • Gastritis, pernicious anemia, gastric surgery, polyps • Immediate family dx gastric cancer • Blood type
Physical Assessment • Early gastric cancer • Indigestion • Abdominal discomfort initially relieved with antacids • Feeling of fullness • Epigastric, back, or retrosternal pain • NOTE: most people will show no clinical manifestations
Physical Assessment cont. • Advanced stage: • Nausea/vomiting • Obstructive symptoms • Iron deficiency/anemia • Palpable epigastric mass • Enlarged lymph nodes • Weakness/fatigue • Progressive weight loss
Labs • Decreased hematocrit and hemoglobin • Macrocytic or microcytic anemia (decreased vit.B12 and iron absorption) • Stool positive for occult blood In Advanced stages: • Hypoalbuminemia • Bilirubin and alkaline phosphate will be abnormal • Increased level of carcinoembryonic antigen
Radiographic assessment • Double contrast upper GI series • C.T. • Esophagogastroduodenoscopy (EGD) • Endoscopic ultrasound (EUS) • Other findings include • Polypoid mass • Ulcer crater • Thickened fibrotic gastric wall
Interventions • Meds: chemotherapy • Fluruorouracil (5-FU) • Doxorubicin • Mitomycin-C • Cisplatin • Etopide (best results when used in combination with each other) Side Effects include nausea/vomiting and bone marrow suppression
Interventions cont. • Radiation • Used most commonly for pre-op • Used in specific hospitals for intra-op • Does not increase survival after operations Side Effects include skin integrity, fatigue, anorexia, and diarrhea
Surgical Interventions • Surgery is the preferred method of treatment • Curative: Total gastrectomy Subtotal gastrectomy • Palliative: To relieve patients pain and ease their suffering
Nursing Interventions • Teach: • s/s of dumping syndrome • Eat small, frequent meals • No liquids with meals (one hour before or after) • Increase protein, fat, and caloric intake • Decrease carbohydrates • Increase Iron, Vit B12, and folate • Dressing changes • Side effects of chemo/radiation • Always provide emotional support
Questions? • True or False: Lab findings have shown stool positive for occult blood, decreased hematocrit and hemoglobin, and hypoalbuminemia in patients with gastric carcinoma • True or False: Most people will show many signs and symptoms indicating gastric cancer • True or False: People who have had gastritis are at a higher risk of developing gastric ca.
Grading Criteria • Joint effort by Elaine M. Lund and Monique Kolin