Download
1 / 31
340 likes | 493 Views
DEVELOPMENT OF THE ENDOCRINE SYSTEM. Prof. Dr. Oya Ercan. Steroid hormones: are not stored rate of synthesis = rate of secretion. Adrenal, gonadal steroids: Synthesis is controlled by trophic hormones.

E N D
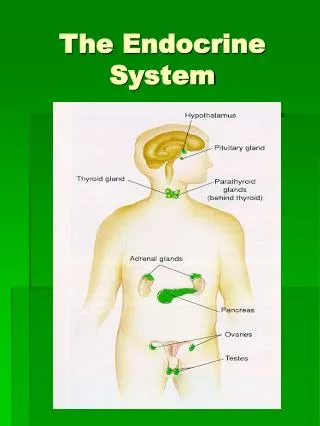
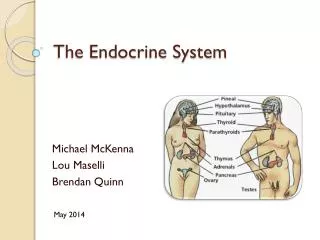
DEVELOPMENT OF THE ENDOCRINE SYSTEM Prof. Dr. Oya Ercan
Steroid hormones: • are not stored • rate of synthesis = rate of secretion
Adrenal, gonadal steroids: • Synthesis is controlled by trophic hormones. Stimulating hormone -------> receptor --------> activation of adenylate cyclase ------> cAMP increases
McCune Albright Syndrome: Mutation in thealpha subunit of G protein. • Testotoxicosis: Mutation of LH receptor ( transmembrane domain - interaction with G protein.)
Syndromes of hormone resistance • Insulin resistance • Testicular feminization • Certain types of dwarfism • Diabeted insipidus (nephrogenic) • Pseudohypoparathyroidism
Hormone ↑ --> receptor number decreases • “down regulation” or “desensitization” • obesity - insulin • precocious puberty - GnRH analogues
Hormone ↑ --> receptor number increases • “up regulation” • estrogen - FSH ↑ ---> LH receptors increase
Distinguishing characteristic of endocrine systems: feedback control & hormone production.
The paradigm for feedback control is the interaction of the pituitary gland with the thyroid, adrenals and gonads. • Hormones produced in peripheral endocrine organs feedback on the hypothalamic-pituitary system ------> regulate the production of the trophic hormones that control peripheral endocrine glands.
All hormones are under some type of feedback control: • by cations (Ca-PTH) • by metabolism (glucose-insulin) • by other hormones • by osmolality or extracellular fluid volume (vasopressin)
Direct Negative Feedback • Metabolite • Cortisol --> ACTH • Thyroid hormones --> TSH
Indirect Negative Feedback • Cortisol --> CRF (corticotropin releasing factor) • Thyroid hormones --> TRH
Short Feedback • TSH --> TRH • ACTH --> CRH
Positive Feedback • Hypophysogonadal (only example) : Estrogen --> LH, FSH
FetalZone • CYP17 (p450c17) --> DHEA --> placentalestrone, estradiol --> DHEAS --> placentalestriol • Sulfotransferase TransitionalZone • CYP17 + 3β HSD --> cortisol OuterDefinitiveZone • 3β HSD --> mineralocorticoids
Fetalcortisol --> cortisone (Midgestation: cortisone (x4-5 cortisol)) • Cortisone: relativelyinactiveglucocorticoid; it protectstheanabolicmilieu of thefetus: cortisol can retardplacentalandfetalgrowth. • As termapproaches; liver, lungexpress 11-ketosteroidreductaseactivity: cortisone--> cortisol • Cortisol: an importantstimulusforpreparingthefetusforextrauterinesurvival.
Insulin-likeGrowthFactors (Somatomedins) Theymediategrowthpromotingaction of GH. • GH is theprimaryregulator of theirplasmalevel. • Theyallhaveinsulin-likeactivity. • Theyaremitogenicforchondrocytes,osteoblastsand a variety of cellsderivedfromextraskeletaltissues. • Theyaretransported in plasmaboundtocarrierproteins → theirhalf life is extended.
Biological Effects • Inadiposetissue, IGF’shavethesamemetabolicactions as insulin but are 1/16th as potent. Theystimulatechondrocyte DNA,RNA,protein,collagenandproteoglycansynthesis. • Theyactprimarily on theskeletaltissues but alsostimulate a widevariety of extraskeletaltissuestogrowanddifferentiate.Theyinducehypoglycemia; on a molarbasis IGF-1 is about 1/16th as potent as insulin in producinghypoglycemia. • Endocrine,paracrine,autocrineactions. • Growthpromotingeffectsthrough IGF receptors;metaboliceffectsthroughinsulinreceptors.
IGF-1 is lowest at birth and rises progressively throughout childhood.After puberty,plasma IGF level falls to normal adult values. • The major regulator of IGF-1 level in serum after birth is GH. Nutritional status is also very important (Malnutrition→IGF↓). There is a decline of about 30% during sleep (sleep associated secretion of GH?).
IGFBPs IGFBP-1 = 27500 dalton GH, IGF-1→upregulate IGFBP3 ↘downregulate IGFBP1
Themorning IGFBP-1(peaklevelsduringthenightand a nadir duringtheday) levelsareage-dependent. • Duringchildhood,a significantinverserelation is foundbetween IGFBP-1 concentrationandchronologicalage. • Thispattern is theopposite of thatfoundfor total IGF-1 andfor IGFBP-3.IGFBP-1 mayact as a transport protein for IGF-1 and IGF-2 fromthecirculationtotheirtargetcells.
IGFBP-3 in thecirculationhave beenproposedtoassure a constantsupply of IGFsfrom a storagepool.Furthermore,BP-3 preventstheinsulin-likeaction of IGFsandprotectsagainsthypoglycemia. • Thelevels of circulation IGFBP-3 in healthysubjectsshow an age-dependentpatternsimilartothatreportedfor IGF-1. IGFBP-3 level is equimolarwiththe total IGF-1 plus IGF-2 concentrationsuggestingthatall IGFBP-3 in circulation is saturatedwith IGF-3. • Thelevelsaredecreased in GH deficiency.
FETAL ZONE • CYP 17 (p450c17) DHEA , DHEAS • Sulfotransferase PlacentaPlacenta estrone estriol estradiol