Download
1 / 17
170 likes | 349 Views
The Impact of ACT Training on Stress and Burnout in Human Services Workers. Jo Lloyd BSc MSc ( j.lloyd@gold.ac.uk ) Professor Frank Bond BA MSc PhD CPsychol. CBT and Individual Focussed Stress-Management.

E N D
The Impact of ACT Training on Stress and Burnout in Human Services Workers Jo Lloyd BSc MSc (j.lloyd@gold.ac.uk) Professor Frank Bond BA MSc PhD CPsychol
CBT and Individual Focussed Stress-Management • Historic relationship between the cognitive behaviour therapies (CBTs) and stress management training (SMT) programmes. • Dates back to relaxation techniques that stemmed from Wolpe’s (1958) systematic desensitization during the 1st wave of behaviour therapy. • SMT movement has wholeheartedly embedded 2nd wave CBT technologies, however research into the relevance of newer psychopathology theories to models of occupational health is in its infancy. • During the past 20 years, these ‘newer’ theories of psychopathology have posited individual characteristics that may be applicable to occupational health.
ACT for Stress-Management • Bond & Hayes (2002) adapted the traditional ACT therapeutic approach to fit into a more training-oriented stress management protocol. • It is predicted that by increasing psychological flexibility people will be better able to: • Be mindful of unwanted thoughts (e.g. negative perceptions of clients or themselves), feelings (e.g. anger, frustration), and impulses (e.g. suppression, avoidance). • Identify, prioritise and pursue their values and goals.
Stress-Management Format • Brief group-based training intervention (8-12 people) • Run from standardised training protocols • 2+1 method of delivery (9 hours contact time in total) • Format allows participants to carry out homework assignments in order to encourage application of learned coping strategies. • Participants receive feedback on their efforts during following session. • Effective behaviours learnt in less therapeutic time
Stress-Management Protocols • Training protocols map directly onto clinical goals of ACT: • Creative hopelessness→ questioning workability of stress coping strategies. • Control is the problem → paradox of trying to “get rid of stress”, polygraph metaphor. • Defusion/acceptance → e.g. costs of low willingness (clean vs. dirty discomfort), leaves on the stream exercise, right vs. wrong, observer exercise. • Values based action → e.g. tombstone eulogy, values clarification (work and personal domains), willingness question (promoting goal-directed action). • Willingness as a values-based action → bubble in the road metaphor, goals, actions and barrier clarification, public commitment to values.
ACT/Psychological Flexibility and Employee Wellbeing • Within occupational contexts ACT training has significantly improved: • General mental health and propensity to innovate in a media organisation (Bond & Bunce, 2000) • General mental health largely in high strain individuals working in UK local government (Flaxman & Bond in press) • Psychological flexibility predicts people’s ability to learn new software as well as their mental health and job performance (Bond and Flaxman, 2006) • People with greater psychological flexibility are better able to take advantage of job control opportunities (Bond & Bunce, 2003; Bond & Flaxman 2006; Bond, Flaxman, & Bunce, 2008)
ACT for Professional Burnout and Stigma • Psychological effects of working with difficult clients (entanglement with stigmatizing attitudes) is a key feature of professional burnout. • Hayes, Bissett et al, (2004) compared the impact of ACT, multicultural, and educational training on professional burnout and stigmatizing attitudes amongst drug abuse counselors. • ACT significantly reduced stigma at follow-up and burnout at post-intervention and follow-up.In addition, reductions in burnout at follow-up significantly exceeded those attained through multicultural training. • Changes in the ACT condition were mediated by changes in the believability of stigmatizing attitudes.
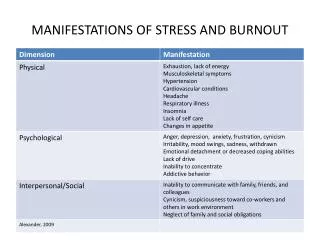
The Human Service Profession • Extending the work of Hayes, Bissett et al (2004) to the human service profession. • Human service workers are often required to spend a considerable proportion of their time in direct involvement with vulnerable people. • Such frequent and emotionally charged interactions can lead to chronic stress and eventually emotional burnout (Maslach, Jackson & Leiter, 1996). • There are a plethora of individual and organisational consequences of stress and emotional burnout.
Present Study • Aim: Investigate the impact of ACT training in improving mental health and performance outcomes among human service workers who deal directly with the elderly. • Design: Randomised controlled outcome experiment comparing two training conditions (1) ACT stress management training (n = 43) and (2) a waitlist control group (n = 67). • Participants: 110 customer-facing staff (sampled nationally) • Outcomes measured at four time points: • T1: pre-training • T2: +1 week (3 hours contact time) • T3: +2 months (6 hours contact time) • T4 :+6 months (9 hours contact time)
Present Study Contd. • Training marketed as “Work-Life Effectiveness Training” • Outcome measures: • Emotional burnout (MBI-HSS) • Psychological distress (GHQ) • Attitude towards the elderly (Kogan’s OP scale) • Job measures (motivation, satisfaction and turnover) • Absenteeism (no. of absences 6 months prior to training, during training and 6 months follow-up). • Mediator variable: • Psychological flexibility (AAQ-II)
Hypotheses • In comparison to a control group, workers who receive ACT training will show significant improvements in mental health and performance outcome measures. • An increase in psychological flexibility will serve as the mechanism by which these changes will occur.
Results: Emotional Exhaustion Non significant T1 → T4 (overall) group X time interaction effect. Significant T2 → T3 group X time interaction effect. ACT: η² = .12 Control: Non sig
Depersonalisation (MBI_DP) Code_num 1.80 training control 1.70 1.60 Scores 1.50 1.40 1.30 T1 T2 T3 T4 Figure 2. Changes in depersonalisation in each condition Results: Depersonalisation Significant T1 → T4 (overall) group X time interaction effect ACT: η² = .32 Control: Non sig Significant T3 → T4 group X time interaction effect. ACT: η² = .19 Control: Non sig
Results: Psychological Distress Significant T1 → T4 (overall) group x time interaction effect ACT: η² = .32 Control: η² = .21 Significant T2 → T3 group X time interaction effect. ACT: η² = .19 Control: η² = .18
Psychological flexibility a b ACT Psychological distress c An increase in psychological flexibility partially mediated the decrease in psychological distress in the ACT group. Results: Mediation Analysis • A series of linear multiple regressions were carried out according to a procedure detailed by Baron and Kenny (1986) to determine mediation.
Conclusions/Implications • ACT training useful in alleviating two emotional burnout components and psychological distress in human service workers. • Mechanism of change for psychological distress was consistent with the core underlying theory of ACT. • No significant change in performance and attitude outcomes. • Critical reductions in negative psychological outcomes can be isolated as occurring at different time points. • Limitations of longitudinal research • Implications for continued support • Burnout patterns (Hatinen, Kinnunen, Pekkonen & Aro, 2004). • Limitation of the long-term utility of interventions focussing only on modifying the individuals coping strategies, without also targeting the toxins inherent in their work environment.