Download
1 / 58
660 likes | 1.12k Views
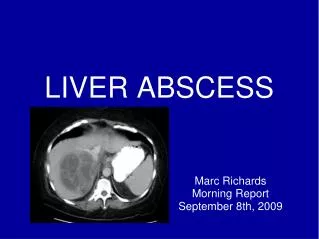
MANAGEMENT OF LIVER ABSCESS. RESHMA RAJ 2002 BATCH. LIVER ABSCESS. 2 TYPES -PYOGENIC -AMOEBIC. PYOGENIC LIVER ABSCESS HISTORY. Described since the time of Hippocrates (4000 BC). 1890 – Osler documented amoebae in stool and abscess of the same patient.

E N D
MANAGEMENT OF LIVER ABSCESS RESHMA RAJ 2002 BATCH
LIVER ABSCESS • 2 TYPES -PYOGENIC -AMOEBIC
PYOGENIC LIVER ABSCESSHISTORY • Described since the time of Hippocrates (4000 BC). • 1890 – Osler documented amoebae in stool and abscess of the same patient. • Dieulafoy described multiple hepatic abscess secondary to pylephlebitis following appendicitis . • In 1938 Ochsner's classic review heralded surgical drainage as the definitive therapy.
INCIDENCE: 0.016% • Majority clinically silent • Peak at 7th decade • Men and women equally affected • Elderly and immunosuppressed more affected • RACE: no role
ETIOLOGY • Biliary causes – 40% -partial or complete obs of biliary tract with ascending cholangitis -biliary manipulations like cholangiography,PCT etc • Portal venous route –20% -perforated Ca colon -diverticulitis -appendicitis with pylephlebitis
Hepatic arterial route –12% -iv drug abuse and its complications -systemic bacteremia -umbilical artery catheterisation -hepatic artery chemoembolisation • Traumatic causes-4% -penetrating trauma to liver -cryosurgical ablation of liver tumors
Direct extension-6% -subphrenic abscess -perforated peptic ulcers -gangrenous cholecystitis • Cryptogenic abscess-20% -asso with DM,malignancy, immunosuppression
Pathology • Usually multiple , small abscesses • More on right lobe of liver BACTERIOLOGY • Staph aureus,Strepto pyogenes,Strepto milleri,strepto faecalis • E coli,Klebsiella,Proteus • Bacteroids,Clostridium,Actinomyces • TB • Fungi-Candida,Aspergillus
CLINICAL FEATURES • SYMPTOMS -Fever (continuous or spiking) - Chills, Malaise - Anorexia,Weight loss -Pain -Nausea and vomiting -Pruritus,Diarrhoea,Cough -PUO
SIGNS -Tenderness in right upper quadrant -Hepatomegaly -Jaundice,right upper quad mass,ascites,pleural effusion
IVESTIGATIONS • LABORATORY -Leucocytosis with shift to left WBC count >10000/mm3 -Anaemia PCV <36% -Hypoalbuminemia Albumin <3g/dl -LFT -ALP
-Gamma glutamyl transpeptidase -Bilurubin >2 gram/dl -SGOT BLOOD CULTURE Aspiration of abscess and C & S
RADIOLOGICAL • X-RAY ABD -Right upper quad gas, air-fluid level in abscess cavity or ileus
USG ABDOMEN -used as a preliminary screen -identify lesions > 2cm in dia -differentiating cystic from solid lesions -diagnosis of gall stones
CT SCAN -investigation of choice -better diagnosis of concurrent or causative pathology -abscess > 0.5 cm in dia -small abscesses near diaphragm and those in fatty liver CONTRAST ENHANCED CT
MRI -lesions as small as 0.3 cm in dia -best for defining hepatic venous anatomy -useful for patients requiring liver resection
NUCLEAR MEDICINE LIVER SCAN Previously used • X-RAY CHEST Right pleural effusion Atelectasis Elevated hemi diaphragm
BARIUM CONTRST STUDIES OF UPPER AND LOWER GIT • Endoscopic retrograde cholangiography/ERC • Per cutaneous cholangiography/PTC
TREATMENT • An untreated hepatic abscess is nearly uniformly fatal due to complications that include sepsis, empyema, or peritonitis from rupture into the pleural or peritoneal spaces, and retroperitoneal extension.
Treatment options • Antibiotics • Aspiration • Percutaneous drainage • Surgical drainage. • Percutaneous drainage plus i.v antibiotics treatment of choice
ANTIBIOTICS • REGIMEN -Broad spectrum synthetic penicillin -Aminoglycoside/3rd gen cephalosporin -Metronidazole • Aminoglycoside toxicity-aztreonam, imipenem • Penicillin allergy-imipenem
Duration of treatment must be individualised • iv antibiotics for 2 weeks • Oral antibiotics for 1 month
Multiple abscesses are more problematic and can require up to 12 weeks of therapy. • Both the clinical and radiographic progress of the patient should guide the length of therapy • FUNGAL ABSCESS – Amphotericin B, Fluconazole
ASPIRATION • Useful in young , otherwise healthy patients with solitary abscess and no co-existing intra-abdominal pathology • Pus can be collected for C & S • Must be radiologically guided
PERCUTANEOUS DRAINAGE • Must be radiologically guided • Most useful for critically ill patients who cannot undergo surgery • Best for solitary, uniseptate abscess • Absolute CI – associated biliary or intra-abdominal pathology, coagulopathy • Relative CI – multiple abscesses and generalised ascites
PROCEDURE • MODIFIED SELDINGER TECHNIQUE • Localise abscess with USG/CT guidance • A 20-gauge teflon sleeve with needle stop is introduced through safest anatomic route possible • Insert a J wire • A no. 8-14 french dialator and then pigtail catheters are advanced over the wire • Abscess evacuated by manual syringe suction • Catheter secured to skin • Catheter irrigated 2-3 times/day with sterile saline • Kept in place till output < 10cc/day or cavity collapse documented by serial CT
SURGICAL DRAINAGE • EXPLORATORY LAPAROTOMY -For diagnosing intra-abdominal pathology -provides concurrent Rx of both abscess and its source -best for multiple abscesses and those inaccessible to PCD, co-existing biliary pathology
EXTRA PERITONEAL APPROACH -subcostal -transpleural -retroperitoneal . Used only for selected abscesses located superiorly in liver dome
TRANSPERITONEAL APPROACH -Standard Rx for patients requiring surgical drainage -Bimanual exmn of liver and intraoperative USG possible -Abscess opened with cautery after localisation -Loculations broken down with finger dissection -Biopsy of abscess wall and nl liver taken -Abscess site irrigated and soft, closed-suction drains placed within abscess cavity in dependent locations
HEPATIC RESECTION • Wedge resection or formal lobectomy -Isolated lobar involvement with single or multiple non healing abscesses -Patients with infected hepatic malignancy -Hemobilia -Chronic granulomatous d/s
LAPAROSCOPIC SURGERY -Limited role -Useful in diagnosing concurrent abd pathology -Laparoscopically guided liver biopsy -Catheter placed under laparoscopic guidance
AMOEBIC LIVER ABSCESS • Tropical and subtropical areas of world are endemic • Early descriptions came from India • Osler reported co-existent hepatic and colonic amoebiasis in 1890 • Exceed PLA in overall frequency
Caused by Entamoeba histolytica • Reaches liver from colon via -Portal vein -Mesenteric lymphatics -Intraperitoneal spread • Incidence : 0.0013% • More among low socioeconomic gps • More among men • Peak at 3rd and 4th decades of life
PATHOLOGY • Abscess usually large, single and superficial • Right lobe usually affected • Fluid interior, inner wall, outer capsule -Abscess fluid resembles “anchovy sauce” -Reddish brown due to digested liver tissue and RBC -Sterile and odourless • Inner wall contains trophozoites-biopsy
CLINICAL FEATURES • Pain, diarrhoea, cough • Shock • Fever and jaundice – less common INVESTIGATIONS Laboratory • LFT abnormalities – less common • PT increase • Stool exmn : cyst and trophozoites -only in 15-50%
SEROLOGY • Indirect hemagglutination test/IHA Gel diffusion precipitin/GDP • Positive if dilutions exceed 1:128 • Result within 24 hrs DIAGNOSTIC ASPIRATION • To r/o PLA when serology is negative • CI in malignancy and echinococcal cyst
RADIOLOGY • USG – Imaging modality of choice • CT Scan – suspecting PLA - Positive serological test with negative hepatic sonogram • MRI • Nuclear medicine liver scan • X-RAY CHEST
USG of amebic abscess-Note peripheral location, rounded shape, poor rim with internal echoes
CT scan of amebic abscess (A). The lesion is peripherally located and round. Rim is nonenhancing but shows peripheral edema (black arrows). Note the extension into the intercostal space (white arrows).
TREATMENT • ANTIBIOTICS • Most uncomplicated amebic liver abscesses can be treated successfully with amebicidal drug therapy alone. • After completion of treatment with tissue amebicides, administer luminal amebicides(diloxanide furoate) for eradication of the asymptomatic colonization state. • Failure to use luminal agents can lead to relapse of infection in approximately 10% of patients. • Metronidazole drug of choice for amebic liver abscess (750 mg 3 times a day orally for 10 days) • Alternatives :Emetine(cardiotoxic) ,chloroquine
THERAPEUTIC ASPIRATION • High risk of abscess rupture, as defined by cavity size greater than 5 cm/250ml vol • Left lobe liver abscess, which is associated with higher mortality and frequency of peritoneal leak or rupture into the pericardium • Treatment failure in which pain and fever persists despite 3 days of antibiotics. • When metronidazole is CI – pregnancy • To relieve pressure symptoms
PERCUTANEOUS DRAINAGE • Most useful for pulmonary, peritoneal and pericardial complications • Risk of secondary infection