Download
1 / 78

E N D
<?xml version="1.0"?><AllQuestions><Question><slideID>350</slideID><slideType>Q&A_QSlide</slideType><questionText>Does he meet the definition for sepsis?</questionText><teamScoringFlag></teamScoringFlag><correctValue></correctValue><incorrectValue></incorrectValue></Question><Question><slideID>352</slideID><slideType>Q&A_QSlide</slideType><questionText>What is your first step in management?</questionText><teamScoringFlag></teamScoringFlag><correctValue></correctValue><incorrectValue></incorrectValue></Question><Question><slideID>354</slideID><slideType>Q&A_QSlide</slideType><questionText>What is the best management now?</questionText><teamScoringFlag></teamScoringFlag><correctValue></correctValue><incorrectValue></incorrectValue></Question><Question><slideID>361</slideID><slideType>Q&A_QSlide</slideType><questionText>What is your next step in management of this patient?</questionText><teamScoringFlag></teamScoringFlag><correctValue></correctValue><incorrectValue></incorrectValue></Question><Question><slideID>365</slideID><slideType>Q&A_QSlide</slideType><questionText>Who will win the Super Bowl?</questionText><teamScoringFlag></teamScoringFlag><correctValue></correctValue><incorrectValue></incorrectValue></Question></AllQuestions> <?xml version="1.0"?><Settings><answerBulletFormat>Numeric</answerBulletFormat><answerNowAutoInsert>No</answerNowAutoInsert><answerNowStyle>Explosion</answerNowStyle><answerNowText>Answer Now</answerNowText><chartColors>Use PowerPoint Color Scheme</chartColors><chartType>Horizontal</chartType><correctAnswerIndicator>Checkmark</correctAnswerIndicator><countdownAutoInsert>No</countdownAutoInsert><countdownSeconds>10</countdownSeconds><countdownSound>TicToc.wav</countdownSound><countdownStyle>Box</countdownStyle><gridAutoInsert>No</gridAutoInsert><gridFillStyle>Answered</gridFillStyle><gridFillColor>0,0,0</gridFillColor><gridOpacity>100%</gridOpacity><gridTextStyle>Keypad #</gridTextStyle><inputSource>Response Devices</inputSource><multipleResponseDivisor># of Responses</multipleResponseDivisor><participantsLeaderBoard>5</participantsLeaderBoard><percentageDecimalPlaces>0</percentageDecimalPlaces><responseCounterAutoInsert>No</responseCounterAutoInsert><responseCounterStyle>Oval</responseCounterStyle><responseCounterDisplayValue># of Votes Received</responseCounterDisplayValue><insertObjectUsingColor>Blue</insertObjectUsingColor><showResults>Yes</showResults><teamColors>User Defined</teamColors><teamIdentificationType>None</teamIdentificationType><teamScoringType>Voting pads only</teamScoringType><teamScoringDecimalPlaces>1</teamScoringDecimalPlaces><teamIdentificationItem></teamIdentificationItem><teamsLeaderBoard>5</teamsLeaderBoard><teamName1></teamName1><teamName2></teamName2><teamName3></teamName3><teamName4></teamName4><teamName5></teamName5><teamName6></teamName6><teamName7></teamName7><teamName8></teamName8><teamName9></teamName9><teamName10></teamName10><showControlBar>Slides with Get Feedback Objects</showControlBar><defaultCorrectPointValue>100</defaultCorrectPointValue><defaultIncorrectPointValue>0</defaultIncorrectPointValue><chartColor1>187,224,227</chartColor1><chartColor2>51,51,153</chartColor2><chartColor3>0,153,153</chartColor3><chartColor4>153,204,0</chartColor4><chartColor5>128,128,128</chartColor5><chartColor6>0,0,0</chartColor6><chartColor7>0,102,204</chartColor7><chartColor8>204,204,255</chartColor8><chartColor9>255,0,0</chartColor9><chartColor10>255,255,0</chartColor10><teamColor1>187,224,227</teamColor1><teamColor2>51,51,153</teamColor2><teamColor3>0,153,153</teamColor3><teamColor4>153,204,0</teamColor4><teamColor5>128,128,128</teamColor5><teamColor6>0,0,0</teamColor6><teamColor7>0,102,204</teamColor7><teamColor8>204,204,255</teamColor8><teamColor9>255,0,0</teamColor9><teamColor10>255,255,0</teamColor10><displayAnswerImagesDuringVote>Yes</displayAnswerImagesDuringVote><displayAnswerImagesWithResponses>Yes</displayAnswerImagesWithResponses><displayAnswerTextDuringVote>Yes</displayAnswerTextDuringVote><displayAnswerTextWithResponses>Yes</displayAnswerTextWithResponses><questionSlideID></questionSlideID><controlBarState>Expanded</controlBarState><isGridColorKnownColor>True</isGridColorKnownColor><gridColorName>Yellow</gridColorName><AutoRec></AutoRec><AutoRecTimeIntrvl></AutoRecTimeIntrvl><chartVotesView>Percentage</chartVotesView><chartLabelsColor>0,0,0</chartLabelsColor><isChartLabelColorKnownColor>True</isChartLabelColorKnownColor><chartLabelColorName>Black</chartLabelColorName><chartXAxisLabelType>Full Text</chartXAxisLabelType></Settings> <?xml version="1.0"?><AllAnswers><Answers><slideID>350</slideID><answerID>0</answerID><answerText>Yes</answerText><isCorrect>None</isCorrect><pointValue>0</pointValue></Answers><Answers><slideID>350</slideID><answerID>1</answerID><answerText>No</answerText><isCorrect>None</isCorrect><pointValue>0</pointValue></Answers><Answers><slideID>350</slideID><answerID>2</answerID><answerText>Not Sure</answerText><isCorrect>None</isCorrect><pointValue>0</pointValue></Answers><Answers><slideID>351</slideID><answerID>0</answerID><answerText>No</answerText><isCorrect>None</isCorrect><pointValue>0</pointValue></Answers><Answers><slideID>352</slideID><answerID>0</answerID><answerText>Bolus with 1 liter IV fluids and monitor for EGD therapy and then administer Vancomycin after blood cultures obtained.</answerText><isCorrect>None</isCorrect><pointValue>0</pointValue></Answers><Answers><slideID>352</slideID><answerID>1</answerID><answerText>Bolus with 1 liter IV fluids and monitor to achieve EDG therapy and administer Cefepime, Ciprofloxacin and Vancomycin.</answerText><isCorrect>None</isCorrect><pointValue>0</pointValue></Answers><Answers><slideID>352</slideID><answerID>2</answerID><answerText>Bolus with 1 liter IV fluids and monitor to achieve EDG therapy and send patient to get CT head prior to LP.</answerText><isCorrect>None</isCorrect><pointValue>0</pointValue></Answers><Answers><slideID>352</slideID><answerID>3</answerID><answerText>Obtain blood cultures from Port and then start Cefepime, Ciprofloxacin, Vancomycin.</answerText><isCorrect>None</isCorrect><pointValue>0</pointValue></Answers><Answers><slideID>353</slideID><answerID>0</answerID><answerText>Bolus with 1 liter IV fluids and monitor to achieve EDG therapy and administer Cefepime, Ciprofloxacin and Vancomycin.</answerText><isCorrect>None</isCorrect><pointValue>0</pointValue></Answers><Answers><slideID>354</slideID><answerID>0</answerID><answerText>These blood cultures are contaminants, therefore disregard, but continue on broad spectrum antibiotics while trying to ID real cause of sepsis.</answerText><isCorrect>None</isCorrect><pointValue>0</pointValue></Answers><Answers><slideID>354</slideID><answerID>1</answerID><answerText>This represents a Central Line associated Blood Stream infection, continue Vancomycin and remove Port.</answerText><isCorrect>None</isCorrect><pointValue>0</pointValue></Answers><Answers><slideID>354</slideID><answerID>2</answerID><answerText>This represents a Central line associated blood stream infection, continue Vancomycin but leave port in place.</answerText><isCorrect>None</isCorrect><pointValue>0</pointValue></Answers><Answers><slideID>355</slideID><answerID>0</answerID><answerText>This represents a Central line associated blood stream infection, continue Vancomycin but leave port in place.</answerText><isCorrect>None</isCorrect><pointValue>0</pointValue></Answers><Answers><slideID>361</slideID><answerID>0</answerID><answerText>Bolus another 1 liter of Normal Saline to achieve goals and then administer epinephrine drip.Bolus another 1 liter of Normal Saline to achieve goals and then administer dopamine drip.Give albumin.</answerText><isCorrect>None</isCorrect><pointValue>0</pointValue></Answers><Answers><slideID>361</slideID><answerID>1</answerID><answerText>Bolus another 1 liter of Normal Saline to achieve goals and then administer dopamine drip.</answerText><isCorrect>None</isCorrect><pointValue>0</pointValue></Answers><Answers><slideID>361</slideID><answerID>2</answerID><answerText>Give albumin.</answerText><isCorrect>None</isCorrect><pointValue>0</pointValue></Answers><Answers><slideID>363</slideID><answerID>0</answerID><answerText>Bolus another 1 liter of Normal Saline to achieve goals and then administer dopamine drip.</answerText><isCorrect>None</isCorrect><pointValue>0</pointValue></Answers><Answers><slideID>365</slideID><answerID>0</answerID><answerText>Denver BroncosNew England PatriotsBaltimore RavensHouston TexansGreen Bay PackersNew York GiantsSan Francisco 49ersNew Orleans Saints</answerText><isCorrect>None</isCorrect><pointValue>0</pointValue></Answers><Answers><slideID>365</slideID><answerID>1</answerID><answerText>New England Patriots</answerText><isCorrect>None</isCorrect><pointValue>0</pointValue></Answers><Answers><slideID>365</slideID><answerID>2</answerID><answerText>Baltimore Ravens</answerText><isCorrect>None</isCorrect><pointValue>0</pointValue></Answers><Answers><slideID>365</slideID><answerID>3</answerID><answerText>Houston Texans</answerText><isCorrect>None</isCorrect><pointValue>0</pointValue></Answers><Answers><slideID>365</slideID><answerID>4</answerID><answerText>Green Bay Packers</answerText><isCorrect>None</isCorrect><pointValue>0</pointValue></Answers><Answers><slideID>365</slideID><answerID>5</answerID><answerText>New York Giants</answerText><isCorrect>None</isCorrect><pointValue>0</pointValue></Answers><Answers><slideID>365</slideID><answerID>6</answerID><answerText>San Francisco 49ers</answerText><isCorrect>None</isCorrect><pointValue>0</pointValue></Answers><Answers><slideID>365</slideID><answerID>7</answerID><answerText>New Orleans Saints</answerText><isCorrect>None</isCorrect><pointValue>0</pointValue></Answers><Answers><slideID>367</slideID><answerID>0</answerID><answerText>Enter your answer options.....</answerText><isCorrect>None</isCorrect><pointValue>0</pointValue></Answers></AllAnswers> Sepsis & Bacteremia John K. Midturi 1/10/2012
Objectives • Understand identification and management of sepsis. • Understand management and treatment of catheter related infections, including indications to remove catheters. • Understand the work up for bacteremia depending on the specific bacteria.
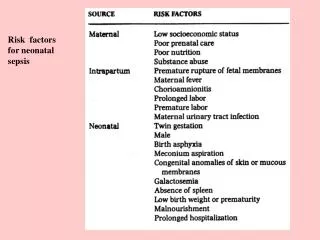
Case • 35 year old male with recent skin trauma from playing flag football. Subjective fevers, and area of cellulitis developed. • Examination: • Temp 37⁰C (99⁰F), HR 88, RR 16, BP 105/75 • Lab: WBC 11000/mm3 http://docfiles.blogspot.com/2006/08/cellulitis-around-leg-abscess.html
Does he meet the definition for sepsis? • Yes • No • Not Sure 0 10
Does he meet the definition for sepsis? No Data filtered on-No
Sepsis: Disease Continuum Infection/Trauma SIRS Sepsis Severe Sepsis • Sepsis with >1 sign of organ failure • Cardiovascular (refractory hypotension) • Renal • Respiratory • Hepatic • Hematologic • CNS • Unexplained metabolic acidosis • Clinical response from nonspecific insult • ≥2 of the following: • Temperature <36⁰ C to >38⁰C • HR > 90beats/min • RR>20breaths/min, PaCO2 <32mmHg • WBC <4000cells/mm3 or >12000/mm3 • or >10% immature neutrophils SIRS with a presumed or confirmed infectious process Bone et al Chest 1992;101:1644
Major cause of morbidity and mortality Worldwide • Leading cause of death in noncoronary ICU (US)1 • 11th leading cause of death overall (US)2 • More than 750,000 cases of severe sepsis in the US annually3 • In the US, more than 500 patients die of severe sepsis daily3 1 Sands KE, et al. JAMA 1997;278:234-40. 2 Murphy SL. National Vital Statistics Reports. 1998. 3 Angus DC, et al. Crit Care Med 2001;29:1303-10.
What can we do about sepsis? http://en.wikipedia.org/wiki/Rosie_the_Riveter
Initial Resuscitation (first 6 hours) • Early Goal Directed Ressuscitation:(Grade 1C) • Central venous pressure (CVP): 8–12mm Hg • Mean arterial pressure (MAP) ≥ 65mm Hg • Urine output ≥ 0.5mL/kg/hr • Central venous (superior vena cava) or mixed venous oxygen saturation ≥ 70% or ≥ 65%, respectively
Reduced 28 day mortality N Engl J Med, Vol. 345, No. 19 November 8, 2001
Initial Resuscitation (first 6 hours) • We suggest(Grade 2C) that if central venous (superior vena cava) or mixed venous oxygen saturation ≥ 70% or ≥ 65% is not achieved with fluid resuscitation • Transfusion of packed red blood cells to achieve a hematocrit >30% or • Dobutamineinfusion (up to a maximum of 20 μg/kg/min)
Diagnosis • Cultures before antibiotics (if no delay in antibiotics) • At least two blood culturesbe obtained prior to antibiotics • Percutaneously (1) and • Each vascular access device (1) • Cultures of other sites • Source of infection-Urine, CSF, Wound, Respiratory secretions, other body fluids • (Grade 1C)
Diagnosis • We recommend that imaging studies be performed promptly in attempts to confirm a potential source of infection. meddean.luc.edu
Initial Resuscitation (first 6 hours) • Antibiotic Therapy • We recommend that intravenous antibiotic therapy be started as early as possible • Within the first hour of recognition of septic shock and severe sepsis without septic shock • We recommend that initial empirical anti-infective • One or more drugs against likely pathogen alsn.mda.org
Case • 65 year old male with history of AML received second round of induction chemotherapy with cytarabine and daunorubicin. He now presents with fever and chills. No SOB, diarrhea, rashes. • Examination: • Temp 39⁰F, BP 90/52, P 112, RR 22 • Confused • Lungs clear • CV- tachycardia • Right subclavian Port without erythema • Labs: • WBC 1.2 • Hgb 9.3 • Platelets 113 • ANC 360
What is your first step in management? • Bolus with 1 liter IV fluids and monitor for EGD therapy and then administer Vancomycin after blood cultures obtained. • Bolus with 1 liter IV fluids and monitor to achieve EDG therapy and administer Cefepime, Ciprofloxacin and Vancomycin. • Bolus with 1 liter IV fluids and monitor to achieve EDG therapy and send patient to get CT head prior to LP. • Obtain blood cultures from Port and then start Cefepime, Ciprofloxacin, Vancomycin. 0 10
What is your first step in management? Bolus with 1 liter IV fluids and monitor to achieve EDG therapy and administer Cefepime, Ciprofloxacin and Vancomycin. Data filtered on-Bolus with 1 liter IV fluids and monitor to achieve EDG therapy and administer Cefepime, Ciprofloxacin and Vancomycin.
Antibiotic Therapy (Grade 2D) • We suggestcombination therapy • known or suspected Pseudomonas infections as a cause of severe sepsis. • neutropenic patients with severe sepsis. • Empirically in patients with severe sepsis, combination therapy should not be administered for more than 3 to 5 days. • De-escalate to single drug therapy.
Antibiotic Therapy • We recommend that the antimicrobial regimen be reassessed daily to: • optimize activity • prevent the development of resistance • reduce toxicity • reduce costs
Antibiotic Therapy • We recommendthat the duration of therapy • 7–10 days (Grade 1D) • Longer courses • Slow clinical response • Un-drainable foci of infection • Immunologic deficiencies including neutropenia • Blood cultures negative in more than 50% of cases of severe sepsis or septic shock (clinical judgment)
Case • 65 year old male with history of AML received second round of induction chemotherapy with cytarabine and daunorubicin. He now presents with fever and chills. No SOB, diarrhea, rashes. • Examination: • Temp 39⁰F, BP 94/54, P 112, RR 22 • Confused • Lungs clear • CV- tachycardia • Right subclavian Port without erythema • Labs: • WBC 1.2 • Hgb 9.3 • Platelets 113 • ANC 360 Blood cultures: Peripheral- Coagulase Negative Staphylococcus @ 2100 Port- Coagulase Negative Staphylococcus @ 1700
What is the best management now? • These blood cultures are contaminants, therefore disregard, but continue on broad spectrum antibiotics while trying to ID real cause of sepsis. • This represents a Central Line associated Blood Stream infection, continue Vancomycin and remove Port. • This represents a Central line associated blood stream infection, continue Vancomycin but leave port in place. 0 10
What is the best management now? This represents a Central line associated blood stream infection, continue Vancomycin but leave port in place. Data filtered on-This represents a Central line associated blood stream infection, continue Vancomycin but leave port in place.
Epidemiology & Pathogenesis • >150million intravascular devices purchased in USA annually • ~80,000 CRBSI in ICUs annually • Short term catheters: <14days • Most CRBSI emanate from insertion site, hub, or both • Long term catheters most prominent source is hub
Definition CRBSI • Bacteremia or fungemia in patient with an intravascular device AND • >1 positive blood culture from peripheral vein • Clinical manifestation of infection (fever/chills/hypotension) • No other source of infection • One of the following: • >15cfu by semiquantitative method or 100 cfu by quantitative method matching peripheral blood culture • Quantitative cultures 3 times greater then peripheral blood culture • Differential time to positivity (catheter 2 hours before peripheral blood culture turn positive) Clinical Infectious Diseases 2009; 49:1–45
What is the best management now? • A. These blood cultures are contaminants, therefore disregard, but continue on broad spectrum antibiotics while trying to ID real cause of sepsis. • B. This represents a Central Line associated Blood Stream infection, continue Vancomycin and remove Port. • C. This represents a Central line associated blood stream infection, continue Vancomycinbut leave port in place.
So now we have diagnosed a CLABSI, What do we do now?
Most common cause of CRBSI • Percutaneous, noncuffed catheters: • Coagulase Negative Staphylococci, S. aureus, Candida species, and enteric gram-negative bacilli • Surgically implanted catheters/PICC: • Coagulase Negative Staphylococci, Enteric gram-negative bacilli, S. aureus, and P. aeruginosa Conservative Diagnosis of CR-BSI • CID 2007:44 (15 March)
DiagnosisWhen and how should catheter cultures & Bcx be obtained? (All level AI or II) • Culture catheters when they are removed for suspected CRBSI • Catheter cultures should not be obtained routinely Clinical Infectious Diseases 2009; 49:1–45
General Management • Day 1 is first day bcxs are negative (CIII) • Vancomycin recommended empiric therapy in institutions with preponderance of MRSA (AII) • If preponderance of MRSA MIC >2, then use daptomycin (AII) • Linezolid should not be used for empiric therapy (AI) • Gram Negative coverage based on severity of illness (4th gen Ceph/carbapen/B-lact/B-lactamse comb +/- aminogly) (AII)
General Management • Empiric combination coverage for MDR GN bacilli should be used in • Neutropenic patients • Severely ill with sepsis • Patients known to be colonized with such pathogens • Until culture & suscept data available to de-escalate therapy (AII)
General Management • Antibiotic lock therapy should be used for catheter salavage (BII), if no antibiotic lock then administer antibiotics through colonized catheter (CIII)
How Long do we need to treat?General Management • Duration: • 4-6 weeks for • Persistent ( >72hrs p removal) fungemia or bacteremia after catheter removal • IE • Suppurative thrombophlebitis • Pediatric osteomyelitis • S. aureus(AII) • Other pathogens (CIII) • 6-8 weeks for adults with osteomyelitis
What if the organism was…. • Staphylococcus aureus • E. coli • Enterococcus • Candida albicans
Evidence Summary-General management • CRBSI • Antibiotics vs catheter removal • 149/169 (88%) had successful microbiologic outcome 1-2 weeks after end of treatment • 83% microbiologic success due to S. aureus • Coagulase-negative Staphylococcus most common cause- most MRSE • There is no compelling data to support specific recommendations for the duration of therapy for device related infections. • Expert Panel Recommendations
Coagulase Negative Staphylococcus species • Uncomplicated CRBSI • 5-7 days if catheter removed • 10-14 days if retained catheter with antibiotic lock (BIII) • Uncomplicated CRBSI • Observe without antibiotics if no intravascular or orthopedic hardware, catheter removed, and additional Bcx negative after catheter removed is negative (CIII) • Staphylococcus lugdunensis CRBSI • Manage same as S. aureus infection (BII)
Staphylococcus aureus • Short term or long term catheters- remove catheter (AII) • If retained • antibiotic lock + systemic x 4 weeks (BII) • Catheter guidewire exchange and replace with antimicrobial impregnated catheter (BII) • Repeat TEE if persistent fever or bacteremia >72 hrs after appropriate antibiotics started & catheter removed if initial TEE negative for endocarditis (AII) • Catheter tip positive for S. aureus but peripheral negative • 5-7 days antibiotics and monitor for signs/symp • additional Bcx (BII) • Replace new catheter when Bcx negative (BII)
Staphylococcus aureusDuration of therapy • Remove infected catheter and 4-6 weeks antibiotics (BII) unless • Not diabetic • Not immunosuppressed- steroids, immuno drugs • Non-neutropenic • Catheter removed • No prosthetic intravascular device-pacemaker, vascular graft • No endocarditis, suppurative thrombophlebitis • Fever resolves w/i 72hrs after antibiotics • No metastatic infection on physical exam Then 2 weeks (AII) • Shorter duration of therapy (2 weeks) should have TEE at least 5-7 days after onset of bacteremia (BII)
Staphylcoccusaureusbacteremia (non-CRBSI) Duration of therapy • Patients receiving 14 days of therapy, including those with catheter-associated bacteremia, had success rates that were lower than those for patients who received a longer course. • Minimum duration of therapy for uncomplicated bacteremia is 2 weeks, as defined by: • (1) Exclusion of endocarditis • (2) No implanted prostheses (eg, prosthetic valves, cardiac devices, and arthroplasties) • (3) Follow-up cultures, 2–4 days after the initial set do not grow MRSA • (4) Defervescencewithin 72 h of therapy • (5) No evidence of metastatic sites of infection
Staphylcoccusaureusbacteremia (non-CRBSI) Duration of therapy • If the above criteria are not met, 4–6 weeks of therapy is recommended for complicated bacteremia depending on the extent of infection; longer durations of therapy may be needed in those who are slow to clear their bacteremia


![Biologics License Application: Recombinant Human Activated Protein C (rhAPC) [drotrecogin alfa (activated)] Xigris ™ f](https://cdn0.slideserve.com/1354659/slide1-dt.jpg)