Download
1 / 47
510 likes | 990 Views
Focus on Status Epilepticus. Joseph I. Sirven, MD On behalf of the American Epilepsy Society Resident, Medical Student, Nursing and Pharmacology Education Committee. History of Status Epilepticus. Xth Marseilles Colloquium (1962)

E N D
Focus on Status Epilepticus Joseph I. Sirven, MD On behalf of the American Epilepsy Society Resident, Medical Student, Nursing and Pharmacology Education Committee
History of Status Epilepticus • Xth Marseilles Colloquium (1962) • Development of modern conceptual basis of status epilepticus (SE) • First meeting devoted to SE • Gastaut
History of Status Epilepticus • Definition • “ a term used whenever a seizure persists for a sufficient length of time or is repeated frequently enough to produce a fixed or enduring epileptic condition.” • … “The fixed and enduring epileptic condition should last at least 30-60 minutes in order to qualify as SE.”
Status Epilepticus Definition • More than 10 minutes of continuous seizure activity or • Two ormore sequential seizures spanning this period without full recovery between seizures
Epidemiological Factors that Impact Outcome/Therapy • Duration of SE = Rapid ID and Treatment • Etiology = Prevention/Neuroprotection • Age = Neuroprotection
Ideal Antiepileptic Drug • Intravenous routes • Few adverse effects • High CNS penetrance • Easy pharmacokinetics • Rapid efficacy
General Measures in SE Management • Maintenance of oxygenation and circulation • Assessment of etiology and lab evaluations • Obtaining intravenous access and initiation of therapy
AEDs for Status epilepticus • Benzodiazepines • Diazepam • Lorazepam • Midazolam • Phenytoin ( Fosphenytoin) • Valproic acid • Phenobarbital
Benzodiazepines • Diazepam (Valium, Diastat) • Lorazepam (Ativan) • Midazolam (Versed)
Diazepam • High lipid solubility • Fast redistribution: 15- 20 minutes • T1/2 elimination: 24 hours • Adverse effects: • respiratory depression • Hypotension • Dose 5-10 mg
Midazolam • Highest lipid solubility • Fast redistribution: 15 minutes • T1/2: 2 hours • Adverse effects: • respiratory depression • Hypotension • Dose:5-10 mg
Lorazepam • Less lipid solubility than Diazepam • Redistribution: 2-3 hours • T1/2 elimination: 6-12 hours • Adverse effects: • respiratory depression • Hypotension • Dose: 4-8 mg
Fosphenytoin • Formulated • Water soluble prodrug • 150 mg/min • IV or IM
Parenteral Valproic Acid • Dose ( Under investigation) • 25 mg/kg dose yields a level 100-150 mg/L in 2-4 hours • Adverse effects • Local irritation • GI distress • Lethargy
Phenobarbital • Dose: 20 mg/kg • Infusion: 100 mg/min • Time to halt seizure: 20-30 min • Duration of action > 48 hours • T ½: 100 hours • AE: sedation, respiratory depression, hypotension
Prehospital Treatment of Status Epilepticus 205 patients enrolled Patient seizing for 5 minutes 3 treatment arms 5 mg valium 2 mg lorazepam 1 ml of propylene glycol/9% NACL Administered by paramedics (after consent from the base hospital)
Prehospital Treatment of Status Epilepticus • Conclusions • Treatment of SE with benzos outside of the hospital are feasible • Lorazepam is likely more effective than diazepam • Lorazepam requires refrigeration
Diazepam vs. Lorazepam • Leppik et. al. 1983 • 78 patients • 10 mg Diazepam vs. 4 mg Lorazepam • Initial Seizure Termination • 58% Diazepam • 78% Lorazepam • P=NS
VA Cooperative Study • Treiman et. al., 1998 • Randomized double blind trial • Four regimens • 0.1 mg/kg lorazepam • 15 mg/kg phenobarbital • 0.15 mg/kg diazepam • 18 mg/kg phenytoin
VA Cooperative Study • 570 patients enrolled • 395 overt • 175 subtle • Primary endpoint: Complete cessation of all seizures within 20 minutes
VA Cooperative Study • Conclusions • Lorazepam is more effective than phenytoin as initial intravenous treatment for overt generalized convulsive SE • Equal efficacy between lorazepam, phenobarbital, diazepam with phenytoin
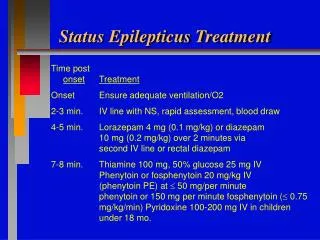
Status Epilepticus Treatment Time post onsetTreatment Onset Ensure adequate ventilation/O2 2-3 min. IV line with NS, rapid assessment, blood draw 4-5 min. Lorazepam 4 mg (0.1 mg/kg) or diazepam 10 mg (0.2 mg/kg) over 2 minutes via second IV line or rectal diazepam 7-8 min. Thiamine 100 mg, 50% glucose 25 mg IV Phenytoin or fosphenytoin 20 mg/kg IV (phenytoin PE) at 50 mg/per minute phenytoin or 150 mg per minute fosphenytoin ( 0.75 mg/kg/min) Pyridoxine 100-200 mg IV in children under 18 mo.
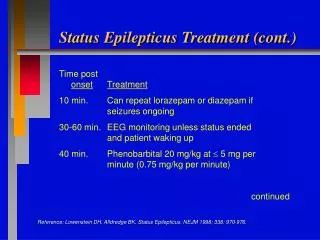
Status Epilepticus Treatment (cont.) Time post onsetTreatment 10 min. Can repeat lorazepam or diazepam if seizures ongoing 30-60 min. EEG monitoring unless status ended and patient waking up 40 min. Phenobarbital 20 mg/kg at 5 mg per minute (0.75 mg/kg per minute) continued Reference: Lowenstein DH, Alldredge BK, Status Epilepticus. NEJM 1998; 338: 970-976.
Status Epilepticus Treatment (cont.) Time post onsetTreatment 70 min. Pentobarbital 3-5 mg/kg load, 1 mg/kg per hour infusion, increase to burst- suppression OR Propofol 3-5 mg/kg load, 5-10 mg/kg/hr initial infusion then 103 mg/kg/hr OR Midazolam 0.2 mg/kg load, .25-2 mg/kg infusion Reference: Lowenstein DH, Alldredge BK, Status Epilepticus. NEJM 1998; 338: 970-976.
Medical Student Cases Case 4: A 62 yo male with Continuous Seizures
Case Study 4 A 62 y/o male without significant previous history of seizures presents to the E R following one generalized tonic-clonic seizure. Initial assessment after the first seizure revealed poorly reactive pupils, no papilledema or retinal hemorrhages and a supple neck.
Case Study 4 Oculocephalic reflex is intact. Respirations are rapid at 22/min and regular, heart rate is 105 with a temperature of 101. As you are leaving the room, the patient had another seizure.
Case Study 4 What should the initial management be? What initial investigations should be performed in this setting? What is the appropriate management with continued seizures if initial therapy does not terminate the seizures?
Case Study 4 Creatinine- 1.0 Mg 1.0 Na- 132 K- 4.5 Ca- 9.0 Glucose- 90 Laboratory study results: CBC WBC- 13.1 HGB 11 Plt 200,000
Case Study 4 What are indications for lumbar puncture in this case? CSF color- clear Cell count tube # 1 – 500 RBC/ 35 WBC- 100% Neutrophils Tube # 3 - 100 RBC/ 11 WBC Protein 65 Glucose 60
Case Study 4 Urinalysis- (+) ketones No White Blood Cells or bacteria Tox screen: negative for alcohol positive for benzodiazepines
Case Study 4 You obtain an MRI of the brain with the following images
Case Study 4 Which of the above studies helps to explain the current seizures? Would you ask for other studies? What are the CSF findings during repeated convulsions?
Case Study 4: Questions to Answer Define Status Epilepticus. Describe the systemic manifestations of status epilepticus. What causes status epilepticus? What is the role of EEG in status epilepticus management?
First AidTonic-Clonic Seizure Turn person on side with face turned toward ground to keep airway clear, protect from nearby hazards Transfer to hospital needed for: • Multiple seizures or status epilepticus • Person is pregnant, injured, diabetic • New onset seizures DO NOT put any object in mouth or restrain
Status Epilepticus A medical emergency • Adverse consequences can include hypoxia, hypotension, acidosis and hyperthermia • Know the recommended sequential protocol for treatment with benzodiazepines, phenytoin, and barbiturates. • Goal: stop seizures as soon as possible