Download
1 / 26
280 likes | 598 Views
RISK OF COLORECTAL CANCER. . . Ulcerative colitis. Control. . . COLORECTAL CANCER RISK IN ULCERATIVE AND CROHN'S COLITIS. . DISTINGUISHING FEATURES OF COLITIS-ASSOCIATED COLORECTAL CANCER. . . FACTORS MODIFYING RISK OF COLITIS-ASSOCIATED CANCER. . . Primary sclerosing cholangitis. Family history of colorectal cancer.

E N D
3. RISK OF COLORECTAL CANCER
4. COLORECTAL CANCER RISK IN ULCERATIVE AND CROHN�S COLITIS 50. COLORECTAL CANCER RISK IN ULCERATIVE AND CROHN�S COLITIS
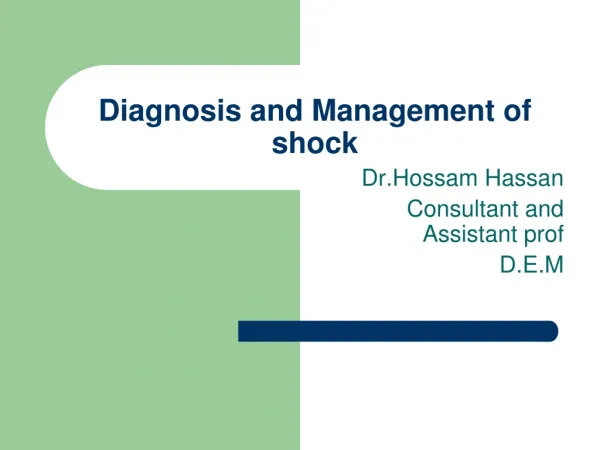
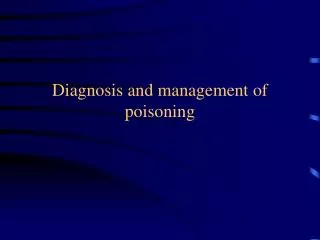
These graphs from a multicenter study comparing the frequency of colorectal cancer in ulcerative and Crohn�s colitis confirm the long-standing but only recently acknowledged suspicion that the cancer risk in the two diseases is virtually identical, given the same duration and anatomical extent of the colitis. (Cf. Fig. 38)
� Gillen CD, Walmsley RS, Prior P, Andrews HA, Allan RN. Ulcerative colitis and Crohn�s disease: a comparison of the colorectal cancer risk in extensive colitis. Gut 1994;35:1590-2.
� Sachar DB. Cancer in Crohn�s disease: dispelling the myths. Gut 1994;35:1507-8.50. COLORECTAL CANCER RISK IN ULCERATIVE AND CROHN�S COLITIS
These graphs from a multicenter study comparing the frequency of colorectal cancer in ulcerative and Crohn�s colitis confirm the long-standing but only recently acknowledged suspicion that the cancer risk in the two diseases is virtually identical, given the same duration and anatomical extent of the colitis. (Cf. Fig. 38)
� Gillen CD, Walmsley RS, Prior P, Andrews HA, Allan RN. Ulcerative colitis and Crohn�s disease: a comparison of the colorectal cancer risk in extensive colitis. Gut 1994;35:1590-2.
� Sachar DB. Cancer in Crohn�s disease: dispelling the myths. Gut 1994;35:1507-8.
5. DISTINGUISHING FEATURES OF COLITIS-ASSOCIATED COLORECTAL CANCER 39. DISTINGUISHING FEATURES OF COLITIS-ASSOCIATED COLORECTAL CANCER
While spontaneous colorectal cancers are synchronously multiple in only about 3% of cases, in ulcerative colitis this figure has been reported as high as 12%. Spontaneous colorectal cancers generally arise from pre-existing adenomatous polyps, but colitis-associated cancers tend to emerge directly from flat mucosa. More extensive infiltration along the bowel wall and a higher frequency of mucinous cytology also characterize colitis-associated cancers. A particularly striking feature of colitis-associated cancer is its occurrence at a mean age two or three decades younger than colorectal cancer in the non-colitis population. All these features suggest that colitis-associated colorectal cancer is a distinct pathogenetic entity, probably attributable to the effects of chronic inflammation and epithelial regeneration. Whatever the biological distinctions may be, however, the disturbing clinical fact remains that colorectal cancer in colitis patients cannot be reliably detected by standard population-based screening methods, and its usual signs and symptoms are likely to be masked by the underlying disease, which leads to a more advanced stage of tumor with resultant poorer prognosis than sporadic colon cancer in the absence of screening for dysplasia.
� Greenstein AJ, Sachar DB, Pucillo A et al. Cancer in universal and left-sided ulcerative colitis: clinical and pathological features. Mt. Sinai J Med 1979;46:25-32.39. DISTINGUISHING FEATURES OF COLITIS-ASSOCIATED COLORECTAL CANCER
While spontaneous colorectal cancers are synchronously multiple in only about 3% of cases, in ulcerative colitis this figure has been reported as high as 12%. Spontaneous colorectal cancers generally arise from pre-existing adenomatous polyps, but colitis-associated cancers tend to emerge directly from flat mucosa. More extensive infiltration along the bowel wall and a higher frequency of mucinous cytology also characterize colitis-associated cancers. A particularly striking feature of colitis-associated cancer is its occurrence at a mean age two or three decades younger than colorectal cancer in the non-colitis population. All these features suggest that colitis-associated colorectal cancer is a distinct pathogenetic entity, probably attributable to the effects of chronic inflammation and epithelial regeneration. Whatever the biological distinctions may be, however, the disturbing clinical fact remains that colorectal cancer in colitis patients cannot be reliably detected by standard population-based screening methods, and its usual signs and symptoms are likely to be masked by the underlying disease, which leads to a more advanced stage of tumor with resultant poorer prognosis than sporadic colon cancer in the absence of screening for dysplasia.
� Greenstein AJ, Sachar DB, Pucillo A et al. Cancer in universal and left-sided ulcerative colitis: clinical and pathological features. Mt. Sinai J Med 1979;46:25-32.
6. FACTORS MODIFYING RISK OF COLITIS-ASSOCIATED CANCER 41. FACTORS MODIFYING RISK OF COLITIS-ASSOCIATED CANCER
It has long been recognized that long duration and wide anatomical extent of colitis are the two principal factors contributing to increased risk of colitis-associated colorectal cancer. More recently, a positive family history of colorectal cancer has been identified as an additive risk factor, much as it is in the non-colitis population. The co-existence of colitis with primary sclerosing cholangitis also sharply increases the likelihood of dysplasia and carcinoma of the colon. Although it is not entirely clear whether the reasons for this observation are primarily biological or artifactual, the fact remains that colorectal cancer surveillance needs to start soon after the diagnosis of PSC-associated colitis. (See Fig. 38)
On the other side of the coin, there is also some evidence suggesting that aminosalicylate treatment, folate supplementation, and �tight� medical control of the inflammatory process might lower the long-term risks of colorectal cancer in ulcerative colitis.
� Shetty K, Rybicki L, Brzezinski A et al. The risk of cancer or dysplasia in ulcerative colitis patients with primary sclerosing cholangitis. Am J Gastroenterol 1999;94:1643-9
� Itzkowitz SH. Inflammatory bowel disease and cancer. Gastroenterol Clin North Am 1997;26:129-39.
� Askling J, Dickman PW, Karlen P et al. Family history as a risk factor for colorectal cancer in IBD. Gastroenterology 2001;120:1356-62.41. FACTORS MODIFYING RISK OF COLITIS-ASSOCIATED CANCER
It has long been recognized that long duration and wide anatomical extent of colitis are the two principal factors contributing to increased risk of colitis-associated colorectal cancer. More recently, a positive family history of colorectal cancer has been identified as an additive risk factor, much as it is in the non-colitis population. The co-existence of colitis with primary sclerosing cholangitis also sharply increases the likelihood of dysplasia and carcinoma of the colon. Although it is not entirely clear whether the reasons for this observation are primarily biological or artifactual, the fact remains that colorectal cancer surveillance needs to start soon after the diagnosis of PSC-associated colitis. (See Fig. 38)
On the other side of the coin, there is also some evidence suggesting that aminosalicylate treatment, folate supplementation, and �tight� medical control of the inflammatory process might lower the long-term risks of colorectal cancer in ulcerative colitis.
� Shetty K, Rybicki L, Brzezinski A et al. The risk of cancer or dysplasia in ulcerative colitis patients with primary sclerosing cholangitis. Am J Gastroenterol 1999;94:1643-9
� Itzkowitz SH. Inflammatory bowel disease and cancer. Gastroenterol Clin North Am 1997;26:129-39.
� Askling J, Dickman PW, Karlen P et al. Family history as a risk factor for colorectal cancer in IBD. Gastroenterology 2001;120:1356-62.
8. COLONOSCOPIC SURVEILLANCE FOR DYSPLASIA 42. COLONOSCOPIC SURVEILLANCE FOR DYSPLASIA
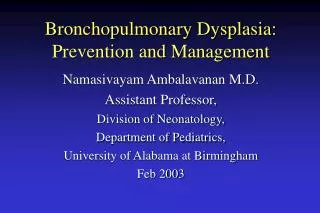
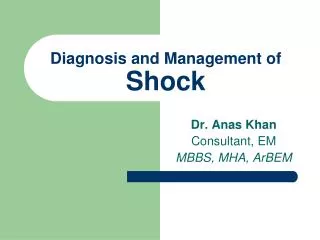
In the search for �early warning signals� of impending malignant transformation, cellular atypia or dysplasia on colonoscopic biopsy has been reported to be a useful sign. Although experience is far from uniform, some series report at least a 50% association of occult malignancy with high-grade dysplasia (lower left panel). For dysplasia to be a reliable warning sign of cancer, however, it is essential that the finding be made independent of severe inflammation (upper left panel). This slide emphasizes the importance, in any program of colonoscopic surveillance for dysplasia, of trying to obtain biopsies from relatively normal areas (solid image in right panel), away from the most grossly inflamed areas of mucosa (dotted image in right panel).
� Riddell RH, Goldman H, Ransohoff DF et al. Dysplasia in inflammatory bowel disease: standardized classification with provisional application. Hum Path 1983;14:931-968.42. COLONOSCOPIC SURVEILLANCE FOR DYSPLASIA
In the search for �early warning signals� of impending malignant transformation, cellular atypia or dysplasia on colonoscopic biopsy has been reported to be a useful sign. Although experience is far from uniform, some series report at least a 50% association of occult malignancy with high-grade dysplasia (lower left panel). For dysplasia to be a reliable warning sign of cancer, however, it is essential that the finding be made independent of severe inflammation (upper left panel). This slide emphasizes the importance, in any program of colonoscopic surveillance for dysplasia, of trying to obtain biopsies from relatively normal areas (solid image in right panel), away from the most grossly inflamed areas of mucosa (dotted image in right panel).
� Riddell RH, Goldman H, Ransohoff DF et al. Dysplasia in inflammatory bowel disease: standardized classification with provisional application. Hum Path 1983;14:931-968.
9. SURVEILLANCE BIOPSY PROTOCOL 48. SURVEILLANCE BIOPSY PROTOCOL
The sensitivity of colonoscopic surveillance for the detection of dysplasia or cancer in colitis is almost surely inadequate unless four-quadrant biopsies are obtained approximately every 10 cm along the entire length of the colon from cecum to rectum.
� Levine DS, Rabinovitch PS, Haggitt RC et al. Distribution of aneuploid cell populations in ulcerative colitis with dysplasia or canceer. Gastroenterology 1991;101:1198-1210.48. SURVEILLANCE BIOPSY PROTOCOL
The sensitivity of colonoscopic surveillance for the detection of dysplasia or cancer in colitis is almost surely inadequate unless four-quadrant biopsies are obtained approximately every 10 cm along the entire length of the colon from cecum to rectum.
� Levine DS, Rabinovitch PS, Haggitt RC et al. Distribution of aneuploid cell populations in ulcerative colitis with dysplasia or canceer. Gastroenterology 1991;101:1198-1210.
11. Chronic Ulcerative Colitis Slide 33. Chronic Ulcerative Colitis
As this term indicates, chronic ulcerative colitis is a lesion with histological evidence of ongoing chronic inflammation without active crypt injury. This may be a manifestation of the natural course of disease in some patients, as active episodes ebb, or it may be the result of treatment, with suppression of the active crypt inflammation. As this slide emphasizes, typical chronic disease exhibits several, if not all, of the features of chronic injury, including atrophy, crypt architecture distortion and a persistent basal or diffuse mucosal lymphoplasmacytic inflammatory infiltrate.Slide 33. Chronic Ulcerative Colitis
As this term indicates, chronic ulcerative colitis is a lesion with histological evidence of ongoing chronic inflammation without active crypt injury. This may be a manifestation of the natural course of disease in some patients, as active episodes ebb, or it may be the result of treatment, with suppression of the active crypt inflammation. As this slide emphasizes, typical chronic disease exhibits several, if not all, of the features of chronic injury, including atrophy, crypt architecture distortion and a persistent basal or diffuse mucosal lymphoplasmacytic inflammatory infiltrate.
12. Chronic Quiescent Ulcerative Colitis Slide 34. Chronic Quiescent Ulcerative Colitis
When chronic injury patterns (architecture distortion, crypt atrophy and mucosa fibrosis) are not attended by significant active or chronic inflammation, the disease is said to be quiescent. Again, this may be an episode in the natural course of disease, or the result of effective treatment. Quiescent disease is usually diagnosed in the context of chronic injury, because only with the latter is there objective evidence of prior involvement of the site sampled by biopsy. It is conceivable that quiescent disease may settle on areas not previously subjected to significant mucosal injury (and remember here that activity without chronicity is not typically encountered in established ulcerative colitis), but in this setting, the difference between quiescent colitis and normal mucosa is a matter of faith, predicated on the previous demonstration of active disease in this site or the good word of a trusted endoscopist with knowledge of the patient�s disease history. Nonetheless, the finding of normal mucosa throughout the colon and rectum in a patient said to have ulcerative colitis (even with prior biopsy evidence of active crypt injury) is less likely quiescent disease than good reason to reconsider the original diagnosis.
It should be emphasized (since it is not illustrated in this slide set) that the features of chronic colitis and chronic quiescent disease might also be seen in biopsies from patients with Crohn�s disease as well. Also, because of the focality of the active lesions in Crohn�s disease, even within affected segments, the presence of normal mucosa in surveillance biopsies may be an expected phenomenon, although evidence of chronic quiescent disease should be demonstrable in other sites or biopsy samples.Slide 34. Chronic Quiescent Ulcerative Colitis
When chronic injury patterns (architecture distortion, crypt atrophy and mucosa fibrosis) are not attended by significant active or chronic inflammation, the disease is said to be quiescent. Again, this may be an episode in the natural course of disease, or the result of effective treatment. Quiescent disease is usually diagnosed in the context of chronic injury, because only with the latter is there objective evidence of prior involvement of the site sampled by biopsy. It is conceivable that quiescent disease may settle on areas not previously subjected to significant mucosal injury (and remember here that activity without chronicity is not typically encountered in established ulcerative colitis), but in this setting, the difference between quiescent colitis and normal mucosa is a matter of faith, predicated on the previous demonstration of active disease in this site or the good word of a trusted endoscopist with knowledge of the patient�s disease history. Nonetheless, the finding of normal mucosa throughout the colon and rectum in a patient said to have ulcerative colitis (even with prior biopsy evidence of active crypt injury) is less likely quiescent disease than good reason to reconsider the original diagnosis.
It should be emphasized (since it is not illustrated in this slide set) that the features of chronic colitis and chronic quiescent disease might also be seen in biopsies from patients with Crohn�s disease as well. Also, because of the focality of the active lesions in Crohn�s disease, even within affected segments, the presence of normal mucosa in surveillance biopsies may be an expected phenomenon, although evidence of chronic quiescent disease should be demonstrable in other sites or biopsy samples.
13. Atypia Indefinite for Dysplasia Slide 44. Atypia Indefinite for Dysplasia
In slide 20, the features of reactive/reparative epithelia atypia were detailed. The most important among these were the presence of focally pseudostratified hyperchromatic nuclei with decreased mucin, intensely eosinophilic or amphophilic cytoplasm and increased mitotic activity. These changes, in active chronic inflammatory bowel disease, are by definition superimposed on architecturally distorted crypts. Since all of these features are shared to some extent with the clonal transformation of mucosal epithelium in low-grade dysplasia, the distinction between repair and dysplasia can be problematic. The presence of prominent nucleoli is more typical of reactive change (when compared with low grade, but not high grade dysplasia), and the nucleus:cytoplasm ratio is either not altered significantly in reactive change or is decreased. Nevertheless, there is sufficient overlap between repair and low-grade dysplasia that the latter cannot be reliably diagnosed in settings that favor reaction/repair (i.e., active crypt injury, erosion or ulceration). Hence, the term indefinite for dysplasia is used when the histologic features of low-grade dysplasia are encountered in areas of active inflammation or when epithelial changes not otherwise characteristic of reaction/repair are present. Needless to say, random biopsies in active inflammatory bowel disease are notoriously difficult to diagnose as low-grade dysplasia.
Petras RE: Nonneoplastic intestinal diseases. In: Sternberg SS, ed., Diagnostic Surgical Pathology 3rded. (New York: Raven Press, 1999), pp 1349-1411.
Slide 44. Atypia Indefinite for Dysplasia
In slide 20, the features of reactive/reparative epithelia atypia were detailed. The most important among these were the presence of focally pseudostratified hyperchromatic nuclei with decreased mucin, intensely eosinophilic or amphophilic cytoplasm and increased mitotic activity. These changes, in active chronic inflammatory bowel disease, are by definition superimposed on architecturally distorted crypts. Since all of these features are shared to some extent with the clonal transformation of mucosal epithelium in low-grade dysplasia, the distinction between repair and dysplasia can be problematic. The presence of prominent nucleoli is more typical of reactive change (when compared with low grade, but not high grade dysplasia), and the nucleus:cytoplasm ratio is either not altered significantly in reactive change or is decreased. Nevertheless, there is sufficient overlap between repair and low-grade dysplasia that the latter cannot be reliably diagnosed in settings that favor reaction/repair (i.e., active crypt injury, erosion or ulceration). Hence, the term indefinite for dysplasia is used when the histologic features of low-grade dysplasia are encountered in areas of active inflammation or when epithelial changes not otherwise characteristic of reaction/repair are present. Needless to say, random biopsies in active inflammatory bowel disease are notoriously difficult to diagnose as low-grade dysplasia.
Petras RE: Nonneoplastic intestinal diseases. In: Sternberg SS, ed., Diagnostic Surgical Pathology 3rded. (New York: Raven Press, 1999), pp 1349-1411.
14. REACTIVE ATYPIA 43. REACTIVE ATYPIA
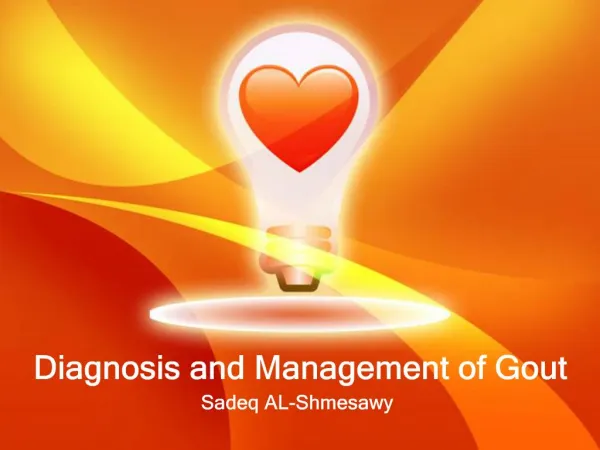
The nuclear heterogeneity in this photomicrograph is limited to the area of maximal inflammation and is strictly proportional to the degree of the inflammation, the severity of the cryptitis, and the activity of the resulting epithelial regeneration. Note also that the goblet cells have retained most of their mucin.43. REACTIVE ATYPIA
The nuclear heterogeneity in this photomicrograph is limited to the area of maximal inflammation and is strictly proportional to the degree of the inflammation, the severity of the cryptitis, and the activity of the resulting epithelial regeneration. Note also that the goblet cells have retained most of their mucin.
15. Low Grade Dysplasia Slide 43. Low Grade Dysplasia
Compared to age-matched population controls, carcinoma occurs with increased frequency in patients with ulcerative colitis and, to a lesser extent, Crohn�s disease. Risk factors for carcinoma in this group of patients include, but are not limited to, duration of disease more than 10 years; duration less than 10 years in patients older than 45 year of age, low grade and high grade dysplasia, and, interestingly, the presence of backwash ileitis (ostensibly a marker of active pan-colitis). Hence, in the context of this unit, a discussion of dysplasia is warranted.
Dysplasia is a pre-invasive clonal transformation that presumably arises in inflammatory bowel disease (both Crohn�s disease and ulcerative colitis) as a consequence of chronic mucosal injury and repair. It typically occurs in areas of mucosa affected by chronic or active inflammation. For this reason (and for reasons alluded to earlier � slides 26 and 27), Crohn�s disease is less amenable to surveillance by random biopsy. Although it may be argued that aggressive surveillance for changes of dysplasia is also of unproven benefit to ulcerative colitis patients (in part because there is no clear manner of predicting progression from low grade to high grade dysplasia to carcinoma � indeed, some colitis patients may present with carcinoma without morphologic evidence of dysplasia elsewhere in the colon; morphologic changes of dysplasia are uncommon, and often missed endoscopically, or may be absent in follow-up biopsies in patients with established dysplasia) it is nonetheless clear that dysplastic epithelium does occur with increasing frequency in ulcerative colitis patients in a time-dependant manner, that the appearance of low grade dysplasia usually precedes the onset of invasive carcinoma in afflicted individuals, and that the appearance of high grade dysplastic changes strongly correlates with concurrent or subsequent diagnosis of invasive disease. High grade dysplasia is discussed further in slide 45, but it is worth noting that the diagnosis of high grade lesions is relatively straightforward in most cases, given the cytologic and architectural changes that typify this process. Identification of early or low-grade dysplasia is considerably more problematic (a point explored further in slide 44). Although dysplasia may present as a polyp or mass lesion (see below), it is perhaps more likely to occur as a localized morphologic transformation in a mucosa �at risk� (chromosomal instability reproducibly precedes the histologic diagnosis of dysplasia), but without distinctive endoscopic attributes. As a result, low-grade dysplasia is most often encountered in random surveillance biopsies.
The characteristic histologic features of dysplasia (as shown in this image) include nuclear enlargement and hyperchromasia, with irregular nuclear contours and striking size variation (pleomorphism). These nuclear changes (as is also true of adenomas in enterocolonic mucosa) are typically first detected in epithelium of the upper crypt and mucosal surface. The latter attribute, in fact, is necessary for the unequivocal diagnosis of dysplasia. Nuclear stratification is also a feature of low-grade dysplasia, while loss of nuclear polarity is more typically encountered in high-grade lesions.
The dysplasias of inflammatory bowel disease may occasionally be mass forming (as polyps or larger mass lesions), hence the term �dysplasia associated lesion or mass � DALM�. Yet, there is no compelling reason why inflammatory bowel disease patients cannot form small benign neoplasms of mucosa � adenomas � unrelated to their inflammatory disease. Indeed, such sporadic adenomas most certainly occur in these patients. The problem is defining such a lesion as sporadic adenoma and not DALM. The clinical consequences are profound, since adenomas can be managed in the same manner as adenomas in otherwise healthy patients, whereas DALM is a marker (especially in high grade lesions) of a substantial risk for development of malignancy. Can a sporadic adenoma be confidently diagnosed in a patient with inflammatory bowel disease, and what criteria should be used? Lesions can be defined as true sporadic adenomas in two settings: 1) a pedunculated or sessile lesion endoscopically distinct from adjacent mucosa, in an area uninvolved by active or chronic colitis; 2) (a bit more difficult): a pedunculated lesion in areas of inflammation that can be completely excised (are free of adenomatous change at the based of the polyp) and are not flanked by dysplastic lesions in adjacent non-polypoid mucosa. It has been shown that the rate of APC gene mutations (and consequent alterations in b-catenin expression) is lower in colitis-associated dysplasia than in sporadic adenomas, but the diagnostic utility of this observation is uncertain. Similarly, alterations in oncogene expression profiles, p53 protein accumulation, and loss of heterozygosity for 3p and the p16 locus broadly distinguish groups of patient with DALM and sporadic adenoma, but are probably not reliably applied to the evaluation of the individual patient. More importantly, these molecular differences best distinguish non-adenoma-like DALM from sporadic adenoma, whereas adenoma-like DALM more closely resembles sporadic disease. Hence, as a general rule, if it looks like an adenoma endoscopically, and it is neither villous in type nor populated by glands with high-grade dysplasia, then it probably is an adenoma. The primary exception to this rule is when the lesion in question arises in a younger patient (not in the adenoma age group) with a well-documented history of active or chronic disease. As a corollary, if flat adenoma-like changes are encountered in random surveillance biopsies when no endoscopic polypoid abnormality is seen, the lesion should always be regarded as dysplasia.
Bennett RC, Bozdech JM, Farmer RG, Petras RE: �Adenomas� (polyps containing adenomatous dysplasia) in ulcerative colitis: a report of 27 cases. Am J Clin Pathol 1990; 94:500-512.
Heuschen UA, Hinz U, Allemeyer EH, Stein J, Lucas M, Autschbach F, Herfarth C, Heuschen G: Backwash ileitis is strongly associated with colorectal carcinoma in ulcerative colitis. Gastroenterol 2001: 120:841-847.
Nugent FW, Haggitt RC, Gilpin PA: Cancer surveillance and ulcerative colitis. Gastroenterology 1991; 100:1241-1248.
Odze RD, Brown CA, Hartmann CJ, Noffsinger AE, Fogt F: Genetic alterations in chronic ulcerative colitis-associated adenoma-like DALMs are similar to non-colitic sporadic adenomas. Am J Surg Pathol 2000; 24:1209-1216.
Rabinovitch PS, Dziadon S, Brentnall TA, et al.: Pancolonic chromosomal instability precedes dysplasia and cancer in ulcerative colitis. Cancer Res 1999; 59:5148-5153.
Riddell RH, Goldman H, Ransohoff DF, et al.: Dysplasia in inflammatory bowel disease: standardized classification with provisional clinical applications. Hum Pathol 1983; 11:931-968.
Tarmin L, Yin J, Harpaz N, et al.: Adenomatous polyposis coli gene mutations in ulcerative colitis-associated dysplasia and carcinoma versus sporadic colon neoplasms. Cancer Res 1995; 55:2035-2038.
Walsh SV, Loda M, Torres CM, Antonioli D, Odze RD: p53 and beta catenin expression in chronic ulcerative colitis-associated polypoid dysplasias and sporadic adenomas: an immunohistochemical study. Am J Surg Pathol 1999; 23:963-969.Slide 43. Low Grade Dysplasia
Compared to age-matched population controls, carcinoma occurs with increased frequency in patients with ulcerative colitis and, to a lesser extent, Crohn�s disease. Risk factors for carcinoma in this group of patients include, but are not limited to, duration of disease more than 10 years; duration less than 10 years in patients older than 45 year of age, low grade and high grade dysplasia, and, interestingly, the presence of backwash ileitis (ostensibly a marker of active pan-colitis). Hence, in the context of this unit, a discussion of dysplasia is warranted.
Dysplasia is a pre-invasive clonal transformation that presumably arises in inflammatory bowel disease (both Crohn�s disease and ulcerative colitis) as a consequence of chronic mucosal injury and repair. It typically occurs in areas of mucosa affected by chronic or active inflammation. For this reason (and for reasons alluded to earlier � slides 26 and 27), Crohn�s disease is less amenable to surveillance by random biopsy. Although it may be argued that aggressive surveillance for changes of dysplasia is also of unproven benefit to ulcerative colitis patients (in part because there is no clear manner of predicting progression from low grade to high grade dysplasia to carcinoma � indeed, some colitis patients may present with carcinoma without morphologic evidence of dysplasia elsewhere in the colon; morphologic changes of dysplasia are uncommon, and often missed endoscopically, or may be absent in follow-up biopsies in patients with established dysplasia) it is nonetheless clear that dysplastic epithelium does occur with increasing frequency in ulcerative colitis patients in a time-dependant manner, that the appearance of low grade dysplasia usually precedes the onset of invasive carcinoma in afflicted individuals, and that the appearance of high grade dysplastic changes strongly correlates with concurrent or subsequent diagnosis of invasive disease. High grade dysplasia is discussed further in slide 45, but it is worth noting that the diagnosis of high grade lesions is relatively straightforward in most cases, given the cytologic and architectural changes that typify this process. Identification of early or low-grade dysplasia is considerably more problematic (a point explored further in slide 44). Although dysplasia may present as a polyp or mass lesion (see below), it is perhaps more likely to occur as a localized morphologic transformation in a mucosa �at risk� (chromosomal instability reproducibly precedes the histologic diagnosis of dysplasia), but without distinctive endoscopic attributes. As a result, low-grade dysplasia is most often encountered in random surveillance biopsies.
The characteristic histologic features of dysplasia (as shown in this image) include nuclear enlargement and hyperchromasia, with irregular nuclear contours and striking size variation (pleomorphism). These nuclear changes (as is also true of adenomas in enterocolonic mucosa) are typically first detected in epithelium of the upper crypt and mucosal surface. The latter attribute, in fact, is necessary for the unequivocal diagnosis of dysplasia. Nuclear stratification is also a feature of low-grade dysplasia, while loss of nuclear polarity is more typically encountered in high-grade lesions.
The dysplasias of inflammatory bowel disease may occasionally be mass forming (as polyps or larger mass lesions), hence the term �dysplasia associated lesion or mass � DALM�. Yet, there is no compelling reason why inflammatory bowel disease patients cannot form small benign neoplasms of mucosa � adenomas � unrelated to their inflammatory disease. Indeed, such sporadic adenomas most certainly occur in these patients. The problem is defining such a lesion as sporadic adenoma and not DALM. The clinical consequences are profound, since adenomas can be managed in the same manner as adenomas in otherwise healthy patients, whereas DALM is a marker (especially in high grade lesions) of a substantial risk for development of malignancy. Can a sporadic adenoma be confidently diagnosed in a patient with inflammatory bowel disease, and what criteria should be used? Lesions can be defined as true sporadic adenomas in two settings: 1) a pedunculated or sessile lesion endoscopically distinct from adjacent mucosa, in an area uninvolved by active or chronic colitis; 2) (a bit more difficult): a pedunculated lesion in areas of inflammation that can be completely excised (are free of adenomatous change at the based of the polyp) and are not flanked by dysplastic lesions in adjacent non-polypoid mucosa. It has been shown that the rate of APC gene mutations (and consequent alterations in b-catenin expression) is lower in colitis-associated dysplasia than in sporadic adenomas, but the diagnostic utility of this observation is uncertain. Similarly, alterations in oncogene expression profiles, p53 protein accumulation, and loss of heterozygosity for 3p and the p16 locus broadly distinguish groups of patient with DALM and sporadic adenoma, but are probably not reliably applied to the evaluation of the individual patient. More importantly, these molecular differences best distinguish non-adenoma-like DALM from sporadic adenoma, whereas adenoma-like DALM more closely resembles sporadic disease. Hence, as a general rule, if it looks like an adenoma endoscopically, and it is neither villous in type nor populated by glands with high-grade dysplasia, then it probably is an adenoma. The primary exception to this rule is when the lesion in question arises in a younger patient (not in the adenoma age group) with a well-documented history of active or chronic disease. As a corollary, if flat adenoma-like changes are encountered in random surveillance biopsies when no endoscopic polypoid abnormality is seen, the lesion should always be regarded as dysplasia.
Bennett RC, Bozdech JM, Farmer RG, Petras RE: �Adenomas� (polyps containing adenomatous dysplasia) in ulcerative colitis: a report of 27 cases. Am J Clin Pathol 1990; 94:500-512.
Heuschen UA, Hinz U, Allemeyer EH, Stein J, Lucas M, Autschbach F, Herfarth C, Heuschen G: Backwash ileitis is strongly associated with colorectal carcinoma in ulcerative colitis. Gastroenterol 2001: 120:841-847.
Nugent FW, Haggitt RC, Gilpin PA: Cancer surveillance and ulcerative colitis. Gastroenterology 1991; 100:1241-1248.
Odze RD, Brown CA, Hartmann CJ, Noffsinger AE, Fogt F: Genetic alterations in chronic ulcerative colitis-associated adenoma-like DALMs are similar to non-colitic sporadic adenomas. Am J Surg Pathol 2000; 24:1209-1216.
Rabinovitch PS, Dziadon S, Brentnall TA, et al.: Pancolonic chromosomal instability precedes dysplasia and cancer in ulcerative colitis. Cancer Res 1999; 59:5148-5153.
Riddell RH, Goldman H, Ransohoff DF, et al.: Dysplasia in inflammatory bowel disease: standardized classification with provisional clinical applications. Hum Pathol 1983; 11:931-968.
Tarmin L, Yin J, Harpaz N, et al.: Adenomatous polyposis coli gene mutations in ulcerative colitis-associated dysplasia and carcinoma versus sporadic colon neoplasms. Cancer Res 1995; 55:2035-2038.
Walsh SV, Loda M, Torres CM, Antonioli D, Odze RD: p53 and beta catenin expression in chronic ulcerative colitis-associated polypoid dysplasias and sporadic adenomas: an immunohistochemical study. Am J Surg Pathol 1999; 23:963-969.
16. LOW-GRADE DYSPLASIA 44. LOW-GRADE DYSPLASIA
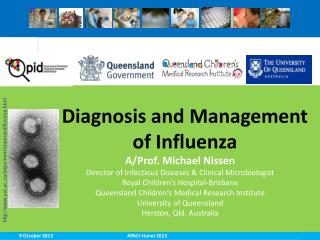
The epithelial cells of the crypts manifest nuclear heterogeneity and �pseudostratification,� often reaching almost to the apex of the cells instead of remaining neatly aligned at the base. These changes are occurring out of proportion to the degree of active inflammation and cryptitis, which are slight at best in this biopsy section.44. LOW-GRADE DYSPLASIA
The epithelial cells of the crypts manifest nuclear heterogeneity and �pseudostratification,� often reaching almost to the apex of the cells instead of remaining neatly aligned at the base. These changes are occurring out of proportion to the degree of active inflammation and cryptitis, which are slight at best in this biopsy section.
17. High Grade Dysplasia Slide 45. High Grade DysplasiaSlide 45. High Grade Dysplasia
18. HIGH-GRADE DYSPLASIA 45. HIGH-GRADE DYSPLASIA
The epithelial cells of the colonic crypts are completely depleted of mucin and have lost their nuclear polarity, to the extent that they seem almost to be arrayed in a sheet rather than arranged in neatly aligned and separated glands.45. HIGH-GRADE DYSPLASIA
The epithelial cells of the colonic crypts are completely depleted of mucin and have lost their nuclear polarity, to the extent that they seem almost to be arrayed in a sheet rather than arranged in neatly aligned and separated glands.
19. Adenocarcinoma in Ulcerative Colitis Slide 46: Adenocarcinoma
If low-grade dysplasia in inflammatory bowel disease is largely a nuclear alteration, high-grade dysplasia can be thought of as both a nuclear and an architectural alteration. Although both lesions may arise in the distorted glands of chronic inflammatory bowel disease, low-grade lesions tend to develop within existing gland profiles, whereas adenoma-like alterations of gland architecture (especially villous in type) typify high-grade dysplasia. Nuclear changes are also more prominent in high-grade disease, with enlarged hyperchromatic and mitotically active nuclei exhibiting complete loss of polarity, even residing at or near the lumenal surface. Nuclear pleomorphism is also more striking in high-grade lesions, and large nuclei with a vesicular chromatin pattern and prominent nucleoli may be seen. Abnormalities have been described in dysplastic mucosa in ulcerative colitis, many of which emphasize the presence of an underlying clonal abnormality in affected mucosa. Although these markers (including p53 accumulation, immunoreactivity for Ki-ras, increased proliferation rates and flow cytometric evidence of altered DNA ploidy) may be of some utility as an adjunct to histologic examination of screening colonoscopic biopsies for the presence or progression of dysplasia, these techniques are not routinely applied in practice and will not be discussed in further detail here.
As shown in slide 46, when architecturally-complex and cytologically-atypical glands otherwise commensurate with high grade dysplasia evoke a desmoplastic stromal response within the lamina propria or deeper tissues, the diagnosis of invasive adenocarcinoma can be entertained. It can be argued that when the biopsy sample is largely effaced by ulceration (admixture of dysplastic elements with stroma may be difficult to distinguish from invasion) or is not representative of submucosal elements (for practical reasons, the general absence of a lymphatic vessels in colorectal mucosa renders the purely intramucosal carcinoma a lesion of at low risk for metastasis at presentation), an unequivocal diagnosis of invasion cannot be rendered. However, I believe that a desmoplastic host response cannot be underestimated as a marker of true extramucosal invasion. Of course, the presence of atypical glands in a desmoplastic stroma in or beneath the muscularis mucosae (as illustrated) is pathognomonic of invasive disease. It should also be recognized that adenocarcinoma in ulcerative colitis (as is also true of high grade dysplasia) may present as a flat lesion, complicating endoscopic detection.
Burmer GC, Rabinovitch PS, Haggitt RC, et al.: Neoplastic progression in ulcerative colitis: histology, DNA content, and loss of a p53 allele. Gastroenterology 1992; 103:1602-1610.
Petras RE: Nonneoplastic intestinal diseases. In: Sternberg SS, ed., Diagnostic Surgical Pathology 3rded. (New York: Raven Press, 1999), pp 1349-1411.
Wong NA, Mayer NJ, MacKell S, Gilmour HM, Harrison DJ: Immunohistochemical assessment of Ki67 and p53 expression assists the diagnosis and grading of ulcerative colitis-related dysplasia. Histopathol 2000; 37:108-114.Slide 46: Adenocarcinoma
If low-grade dysplasia in inflammatory bowel disease is largely a nuclear alteration, high-grade dysplasia can be thought of as both a nuclear and an architectural alteration. Although both lesions may arise in the distorted glands of chronic inflammatory bowel disease, low-grade lesions tend to develop within existing gland profiles, whereas adenoma-like alterations of gland architecture (especially villous in type) typify high-grade dysplasia. Nuclear changes are also more prominent in high-grade disease, with enlarged hyperchromatic and mitotically active nuclei exhibiting complete loss of polarity, even residing at or near the lumenal surface. Nuclear pleomorphism is also more striking in high-grade lesions, and large nuclei with a vesicular chromatin pattern and prominent nucleoli may be seen. Abnormalities have been described in dysplastic mucosa in ulcerative colitis, many of which emphasize the presence of an underlying clonal abnormality in affected mucosa. Although these markers (including p53 accumulation, immunoreactivity for Ki-ras, increased proliferation rates and flow cytometric evidence of altered DNA ploidy) may be of some utility as an adjunct to histologic examination of screening colonoscopic biopsies for the presence or progression of dysplasia, these techniques are not routinely applied in practice and will not be discussed in further detail here.
As shown in slide 46, when architecturally-complex and cytologically-atypical glands otherwise commensurate with high grade dysplasia evoke a desmoplastic stromal response within the lamina propria or deeper tissues, the diagnosis of invasive adenocarcinoma can be entertained. It can be argued that when the biopsy sample is largely effaced by ulceration (admixture of dysplastic elements with stroma may be difficult to distinguish from invasion) or is not representative of submucosal elements (for practical reasons, the general absence of a lymphatic vessels in colorectal mucosa renders the purely intramucosal carcinoma a lesion of at low risk for metastasis at presentation), an unequivocal diagnosis of invasion cannot be rendered. However, I believe that a desmoplastic host response cannot be underestimated as a marker of true extramucosal invasion. Of course, the presence of atypical glands in a desmoplastic stroma in or beneath the muscularis mucosae (as illustrated) is pathognomonic of invasive disease. It should also be recognized that adenocarcinoma in ulcerative colitis (as is also true of high grade dysplasia) may present as a flat lesion, complicating endoscopic detection.
Burmer GC, Rabinovitch PS, Haggitt RC, et al.: Neoplastic progression in ulcerative colitis: histology, DNA content, and loss of a p53 allele. Gastroenterology 1992; 103:1602-1610.
Petras RE: Nonneoplastic intestinal diseases. In: Sternberg SS, ed., Diagnostic Surgical Pathology 3rded. (New York: Raven Press, 1999), pp 1349-1411.
Wong NA, Mayer NJ, MacKell S, Gilmour HM, Harrison DJ: Immunohistochemical assessment of Ki67 and p53 expression assists the diagnosis and grading of ulcerative colitis-related dysplasia. Histopathol 2000; 37:108-114.
20. 46. ADENOMATOUS-LIKE POLYP IN ULCERATIVE COLITIS
The polyp in this colonoscopic photograph from an ulcerative colitis patient will show unmistakable dysplasia on histology, but both grossly and microscopically there is nothing to distinguish it from an ordinary adenomatous polyp that might be found in someone without colitis. So long as the polyp is entirely excised endoscopically, and there is no dysplasia anywhere else in the colon�either adjacent or at a distance on extensive multiple biopsies�recent evidence suggests that the patient can safely be followed with close and continuous surveillance, without automatic resort to colectomy.
� Engelsgjerd M, Farraye FA, Odze RD. Polypectomy may be adequate treatment for adenoma-like dysplastic lesions in chronic ulcerative colitis. Gastroenterology 1999;117:1288-94.
� Rubin PH, Friedman S, Harpaz N et al. Colonoscopic polypectomy in chronic colitis: conservative management after endoscopic resection of dysplastic polyps. Gastroenterology 1999;117:1295-1300.
� Odze RD. Adenomas and adenoma-like DALMs in chronic ulcerative colitis: a clinical, pathological, and molecular review. Am J Gastroenterol 1999;94:1746-50.46. ADENOMATOUS-LIKE POLYP IN ULCERATIVE COLITIS
The polyp in this colonoscopic photograph from an ulcerative colitis patient will show unmistakable dysplasia on histology, but both grossly and microscopically there is nothing to distinguish it from an ordinary adenomatous polyp that might be found in someone without colitis. So long as the polyp is entirely excised endoscopically, and there is no dysplasia anywhere else in the colon�either adjacent or at a distance on extensive multiple biopsies�recent evidence suggests that the patient can safely be followed with close and continuous surveillance, without automatic resort to colectomy.
� Engelsgjerd M, Farraye FA, Odze RD. Polypectomy may be adequate treatment for adenoma-like dysplastic lesions in chronic ulcerative colitis. Gastroenterology 1999;117:1288-94.
� Rubin PH, Friedman S, Harpaz N et al. Colonoscopic polypectomy in chronic colitis: conservative management after endoscopic resection of dysplastic polyps. Gastroenterology 1999;117:1295-1300.
� Odze RD. Adenomas and adenoma-like DALMs in chronic ulcerative colitis: a clinical, pathological, and molecular review. Am J Gastroenterol 1999;94:1746-50.
22. Pseudopolyps Slide 32. Pseudopolyps
In ulcerative colitis, despite its name, loss of surface mucosa (erosion) or full thickness mucosal loss (ulceration) are not macroscopic phenomena, except in fulminant disease, and thus are usually only demonstrated in histological sections. The reason for this is that ulcers are the result of progressive crypt injury and destruction. As the base of an inflamed crypt is destroyed, inflammation may extend laterally at or above the muscularis mucosae, undermining portions of adjacent mucosa. In the course of aggressive active crypt injury, this lateral extension, perhaps incorporating multiple adjacent crypt abscesses, isolates islands of inflamed mucosa. Ongoing inflammation, with reparative and hyperplastic change, edema and granulation tissue, results in expansion of these islands into macroscopically evident polypoid lesions, the so-called �pseudopolyp�. These are not regarded as true polyps, comparable to hyperplastic or neoplastic lesions, because their exophytic nature is not defined by a proliferation from within an intact mucosa, but rather, results from a loss of adjacent tissue. In unusual examples of ulcerative colitis, pseudopolyps may be so numerous and so large that they resemble adenomatous polyposis.Slide 32. Pseudopolyps
In ulcerative colitis, despite its name, loss of surface mucosa (erosion) or full thickness mucosal loss (ulceration) are not macroscopic phenomena, except in fulminant disease, and thus are usually only demonstrated in histological sections. The reason for this is that ulcers are the result of progressive crypt injury and destruction. As the base of an inflamed crypt is destroyed, inflammation may extend laterally at or above the muscularis mucosae, undermining portions of adjacent mucosa. In the course of aggressive active crypt injury, this lateral extension, perhaps incorporating multiple adjacent crypt abscesses, isolates islands of inflamed mucosa. Ongoing inflammation, with reparative and hyperplastic change, edema and granulation tissue, results in expansion of these islands into macroscopically evident polypoid lesions, the so-called �pseudopolyp�. These are not regarded as true polyps, comparable to hyperplastic or neoplastic lesions, because their exophytic nature is not defined by a proliferation from within an intact mucosa, but rather, results from a loss of adjacent tissue. In unusual examples of ulcerative colitis, pseudopolyps may be so numerous and so large that they resemble adenomatous polyposis.
23. DALMS IN ULCERATIVE COLITIS 47. DALMS IN ULCERATIVE COLITIS
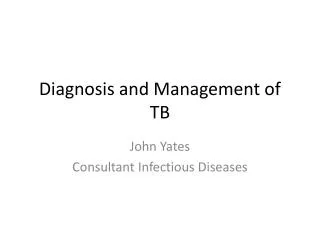
In striking contrast to the pedunculated, completely excisable polyp shown in Figure 46, the finding of any degree of dysplasia in the broad-based, nodular mucosal elevations in these three patients with long-standing ulcerative colitis mandates immediate colectomy on account of the 80%+ risk of synchronous or subsequent carcinoma.
� Blackstone MO, Riddell RH, Rogers BHG et al. Dysplasia-associated lesion or mass (DALM) detected by colonoscopy in long-standing ulcerative colitis: an indication for colectomy. Gastroenterology 1981;80:366-74.47. DALMS IN ULCERATIVE COLITIS
In striking contrast to the pedunculated, completely excisable polyp shown in Figure 46, the finding of any degree of dysplasia in the broad-based, nodular mucosal elevations in these three patients with long-standing ulcerative colitis mandates immediate colectomy on account of the 80%+ risk of synchronous or subsequent carcinoma.
� Blackstone MO, Riddell RH, Rogers BHG et al. Dysplasia-associated lesion or mass (DALM) detected by colonoscopy in long-standing ulcerative colitis: an indication for colectomy. Gastroenterology 1981;80:366-74.